Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
本邦では胃癌あるいは胃手術後に生じた胃横行結腸瘻の報告は少くないが,胃潰瘍を成因とした胃横行結腸瘻は極めて少く,われわれが渉猟した限りでは現在まで9例の報告をみるに過ぎない.最近われわれは胃潰瘍による胃横行結腸痩をX線検査,内視鏡検査などにより確認し手術にて治癒せしめた一例を経験したので報告する.
Since the initial report in 1775 by Haller, gastrocolic fistula, originating from gastric cancer and perforated into the transverse colon, has been described considerably in the U. S. and Europe. However, gastrocolic fistula in a patient without previous abdominal surgery or originating from gastric ulcer is relatively uncommon. In Japan, to date, this disease has been extremely rare, and nine cases only have been reported so far. Its clinical signs and symptoms are chiefly characterized by diarrhoea, weight loss, belching with fecal stink, stercoracious vomitting and malnutrition.
In this paper is presented a recently experienced case of gastrocolic fistula originating from gastric ulcer and perforated into the transverse colon.
A man aged 44 was admitted to our hospital on March 17, 1972, for investigation of diarrhea and abdominal distension which had begun about two years before.
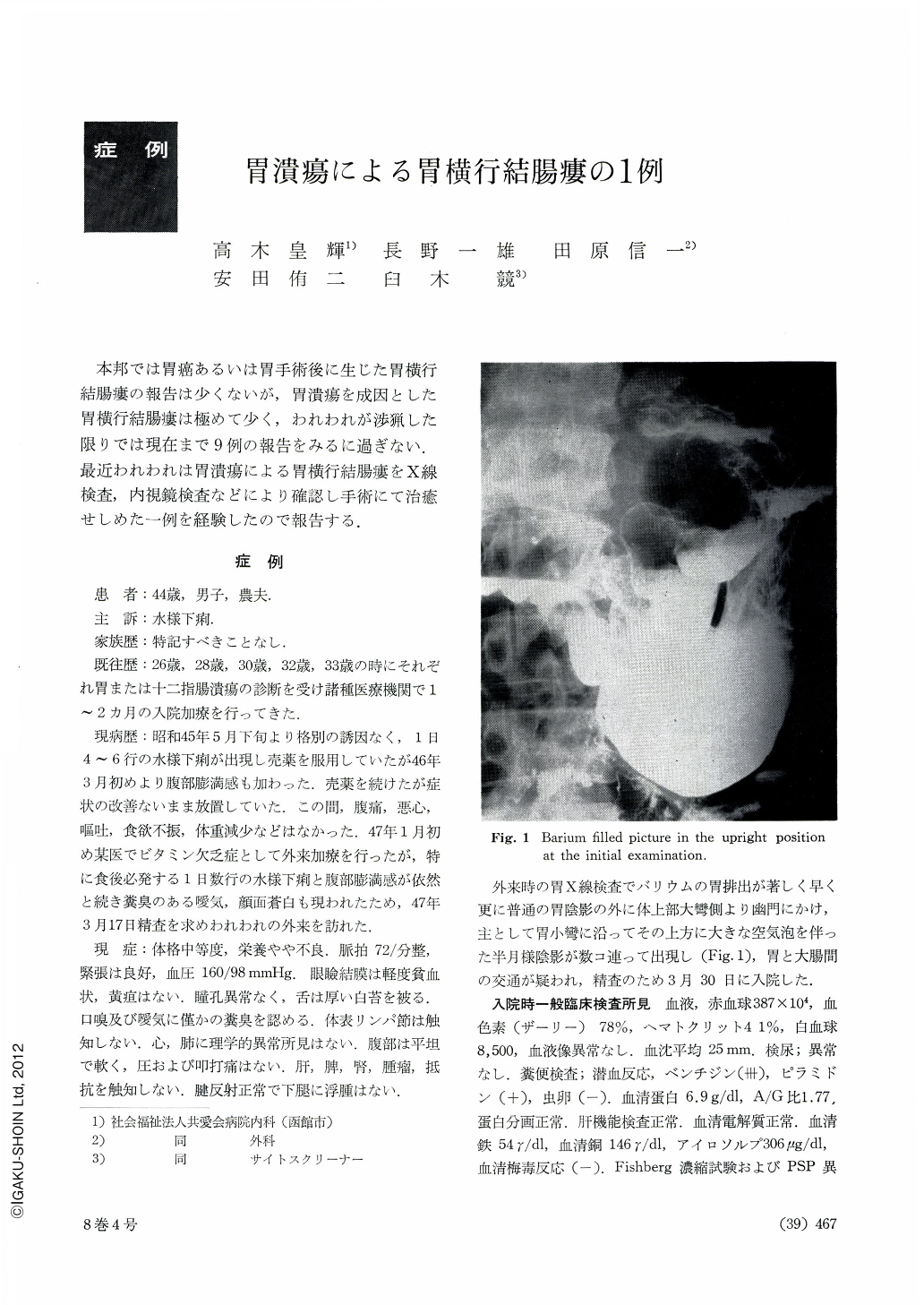
At X-ray study of the stomach, abnormal backward flow of barium was observed from the posterior wall of the prepyloric portion besides the normal barium flow into the doudenum, and its flow showed the haustra directly after it. Many gaseous shadows in the whole abdomen were seen by the plain radiograph. Barium enema examination of the colon showed direct flow of the barium into the stomach from the mid-portion of the transverse colon, revealing distinctly the outline of the stomach. These examinations clearly demonstrated a fistulous communication bestween the stomach and transverse colon. Also at another barium meal study, the contrast medium entering normally into the large intestine regurgitated into the stomach by way of a fistulous lumen, going into the duodenum all over again. Therefore, the barium remained in the gastrointestinal tract for several days.
Gastric endoscopy revealed masses of feces here and there, and demonstrated the orifice of the fistula the size of a forefinger-tip on the posterior wall of the prepyloric portion. The mucosal folds of the transverse colon were observed directly from there. The fistula along with its surrounding area was elevated as a whole, and it aroused a suspicion of perforation of peptic ulcer into the transverse colon. No malignant changes were observed in the stomach. As a further means of ascertaning fistulous communication, we injected methylene blue solution into the rectum as in a barium enema, while watching the gastric lumen with endoscopy, and thus we were able to catch a glimpse of the coloring matter being regurgitated into the stomach from the fistulous tract. We also attempted to insert a cannula into the orifice by means of duodenofiberscope under direct vision. When gastrografin was injected into the fistula, the haustra of the transverse colon were revealed clearly. When we next sent both gastrografin and air through the cannula into the colon, its double contrast picture was seen very well. By these findings we arrived at a preoperative diagnosis of gastrocolic fistula originating from gastric ulcer and perforated into the transverse colon.
The fistulous tract was resected en bloc by subtotal gastrectomy and colectomy.
Gross observation of the resected specimen showed on the posterior wall in the lesser curvature side about 1.5 cm oral from the pyloric ring a perforated ulcer, 1.5×1.5 cm in dimensions, with irregular margins. In the center of the ulcer was a fistulous tract. The colonic opening measured 1.4×1.5 cm. The perforated ulcer along with the surrounding area was elevated as a whole the same as in endoscopic observation, and elevation gradually merged into the encircling normal mucosa. Histologic diagnosis was gastrocolic fistula originated from peptic ulcer of the stomach.
As the diagnosis of this disease is believed to be difficult by roentgenologic and endoscopic studies, it has been here presented with some reference to the literature.
Copyright © 1973, Igaku-Shoin Ltd. All rights reserved.

