Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
腸の虚血状態は,その程度と範囲の差により,各種の腸病変を引き起こすことが知られている.腸間膜動脈などの主幹動脈の閉塞に基づく広範囲な腸壊死は,その代表的な重篤な疾患と言える.しかし最近,病変の範囲も狭く,また変化も軽度で死に至らない大腸の虚血性病変が注目され1),虚血性大腸炎(ischemic colitis)という名称のもとに疾患の概念が確立しつつある2)3).われわれは腹痛,下血,発熱をもって急激に発症し,臨床所見およびその経過,X線像と内視鏡所見より,狭窄型の虚血性大腸炎と診断しうる1例を経験した.しかもこの例について,注腸X線像を経時的に追跡しえたので,そのX線所見の推移を中心に報告する.
症 例
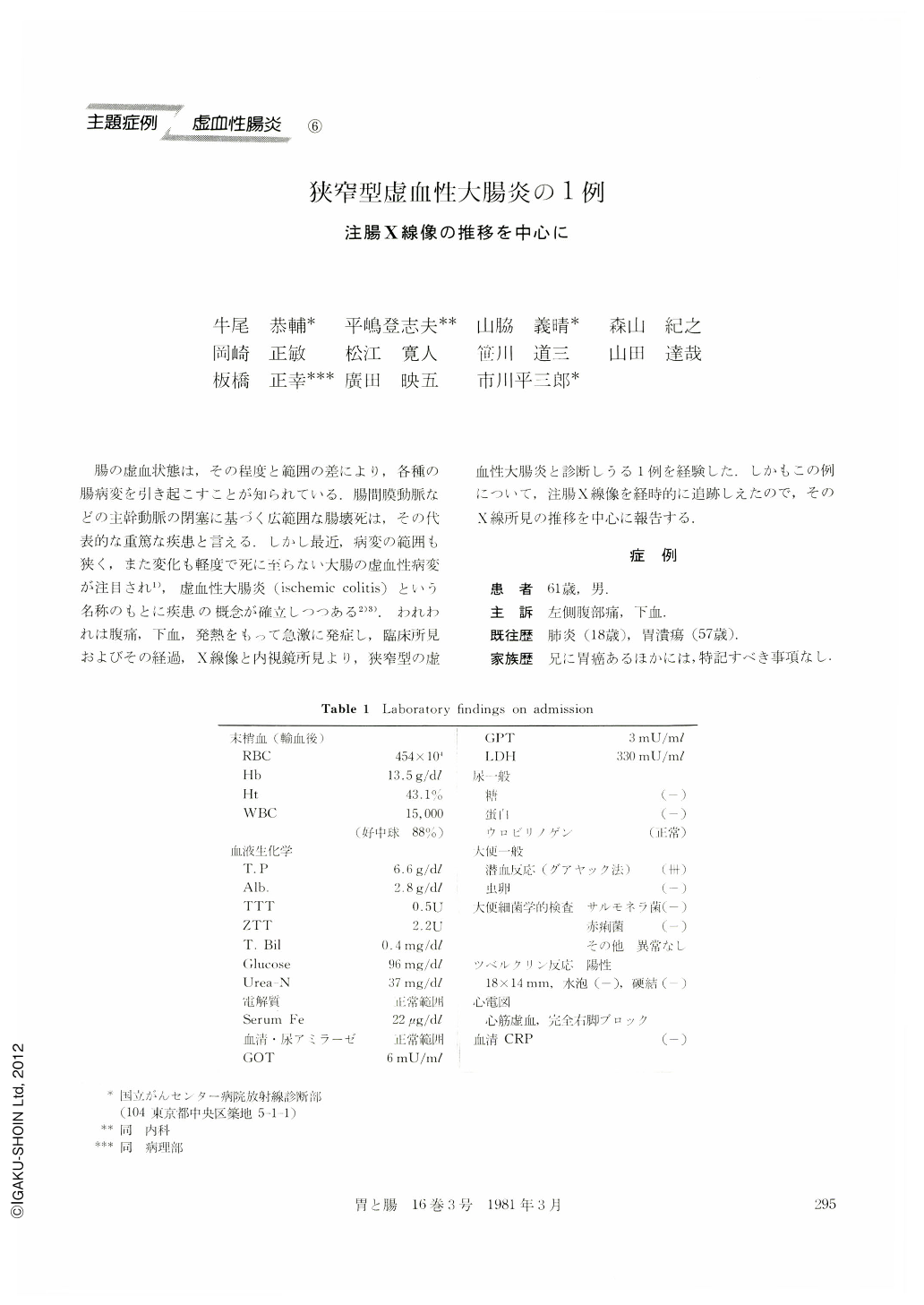
患 者 61歳,男.
主 訴 左側腹部痛,下血.
既往歴 肺炎(18歳),胃潰瘍(57歳).
家族歴 兄に胃癌あるほかには,特記すべき事項なし.
生活歴 外国での居住歴なし,その他特記すべき事項なし.
現病歴 45歳ごろより高血圧を指摘され,某院にて内服治療中であった.1974年の夏ごろより,歩行時に時々,左前胸部の不快感を覚えていたが,2~3分間の安静で消失していた.1974年9月6日より3日間排便がなく,9日の朝,食事後に浣腸したが排便はなかった.正午ごろ,急に悪心嘔吐があり立ち上がれなくなったので,救急車にて某院受診した,そのときの最高血圧は240mmHgであった.午後1時ごろより急に左の下腹部と側腹部痛を認め,午後3時には,便器いっぱいに血餅様の黒色便を排出した.翌10日にも腹痛と下血は続き,疲労感と全身倦
怠感を覚え,通常200mmHgある最高血圧が146mHgに低下したので,11日,車椅子にて国立がんセンター病院に入院した.
A 61 year-old male, who had been pointed out to have hypertension since 16 years ago, was admitted to National Cancer Center Hospital complaining of left abdominal cramp, fever (37.6℃) and diarrhea with massive bleeding. Physical examination revealed severe left quadrant tenderness. On routine laboratory investigation, the white cell count was 15,000 mm3 and hemooccult reaction in feces was three positive. Electrocardiogram showed myocardial ischemia and complete right bundle branch block. The plain x-ray film of the abdomen taken three days after the onset revealed multiple nodular filling defects (thumb printing) throughout the narrowed descending colon.
Diagnosis of ischemic colitis was made on the basis of the clinical, laboratory findings and abdominal plain film. He was treated with antibiotics (penicillin and kanamycin) and symptomatic treatment. The patient's symptoms and signs settled within two weeks, and positive occult blood of feces and leuko cytosis were not seen on the tenth days after the onset. Flexible fiberoptic colonoscopy showed the longitudinal ulcer with white coat. Histological examination of biopsy specimen taken from the ulcer revealed the necrotic granulation tissue with fibrinous exudatives and inflammatory cell infiltration and there were no evidence of any mucosal changes suggesting of ulcerative colitis or chronic specific granulomatous diseases. Barium enema study performed on the 40th days after the onset showed an area of stenosis 20 cm in length in the descending colon with longitudinal ulcer and mucosal irregularity. Repeated barium enema performed on the 118th days after the onset showed the healed ulcer, sacculation and marginal rigidity in the descending colon. Last barium enema conducted on the 223 rd days after the onset showed only the unilateral stricture with sacculation and rigidity, but mucosa appeared to be normal.
From the symptoms of onset, the clinical course, the endoscopic and radiographic examination, this case was considered to be the stricturing form which Marston classified in ischemic colitis.
Copyright © 1981, Igaku-Shoin Ltd. All rights reserved.

