Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
- サイト内被引用 Cited by
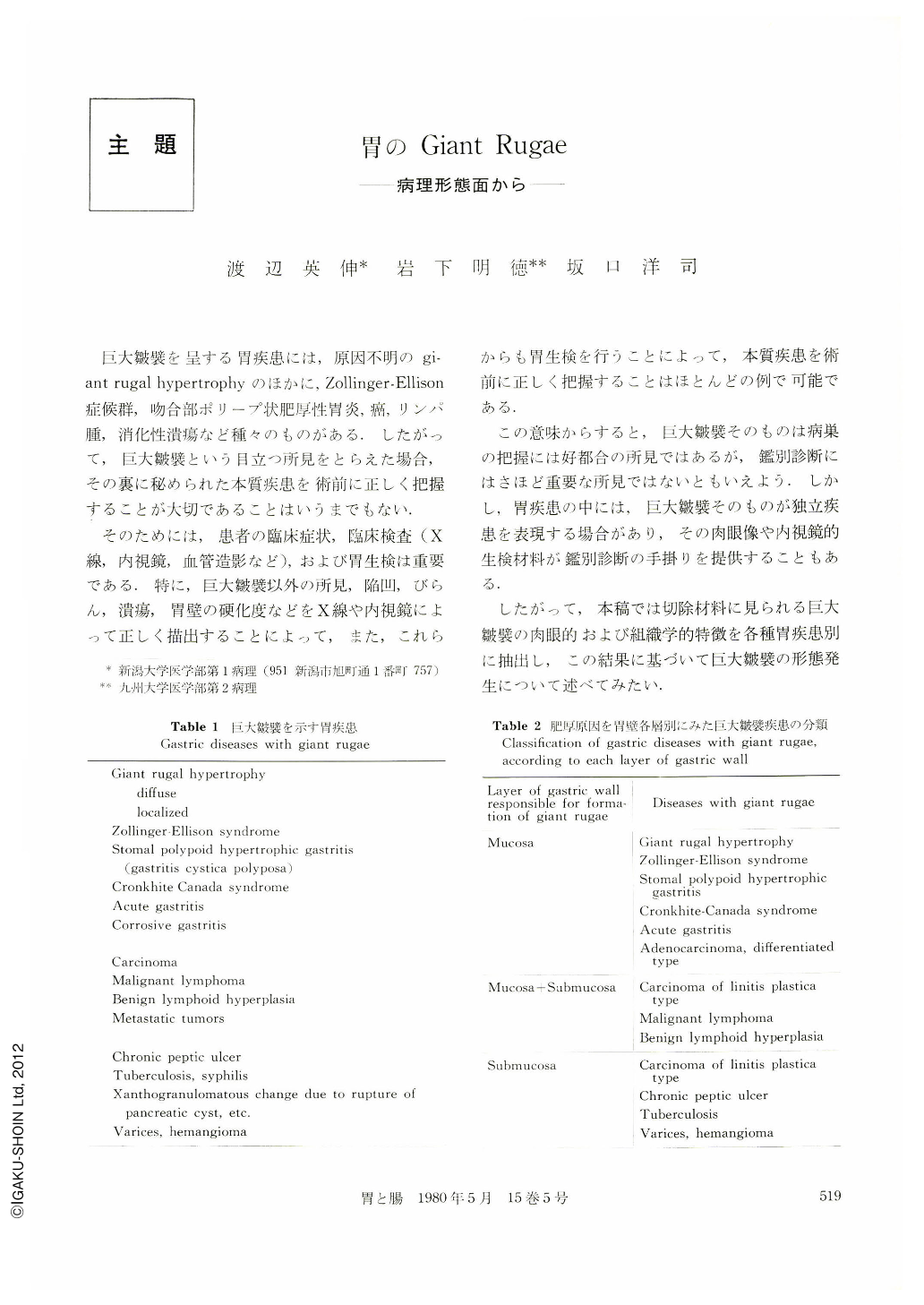
巨大皺襞を呈する胃疾患には,原因不明のgiant rugal hypertrophyのほかに,Zollinger-Ellison症候群,吻合部ポリープ状肥厚性胃炎,癌,リンパ腫,消化性潰瘍など種々のものがある.したがって,巨大皺襞という目立つ所見をとらえた場合,その裏に秘められた本質疾患を術前に正しく把握することが大切であることはいうまでもない.
そのためには,患者の臨床症状,臨床検査(X線,内視鏡,血管造影など),および胃生検は重要である.特に,巨大皺襞以外の所見,陥凹,びらん,潰瘍,胃壁の硬化度などをX線や内視鏡によって正しく描出することによって,また,これらからも胃生検を行うことによって,本質疾患を術前に正しく把握することはほとんどの例で可能である.
We studied on macroscopic and microscopic characteristics of each gastric disease with giant rugae, using resected stomachs with giant rugai hypertrophy (eight cases), stomal poiypoid hypertrophic gastritis (13 cases), Cronkhite-Canada syndrome (one case), malignant lymphoma (five cases), benign lymphoid hyperplasia (11 cases) and multiple ulcers due to rupture of pancreatic cyst into gastric wall (one case) (Table 1).
Macroscopically, giant rugae in each disease differed in distribution, form, surface appearance and rigidity. Microscopically as well, they were different each other and were divided into three groups according to each layer of gastric wall responsible for formation of the giant rugae: mucosa, submucosa and both (Table 2).
Firstly, giant rugae as seen in Fig. consisted of simple hyperplasia of fundic mucosa in giant rugal hypertrophy and Zollinger-Ellison syndrome. The former showed pseudopyloric glands and their cysts in various numbers in each rnucosal area and each case. The latter revealed an increase in number of parietal cells, occasional shortening of foveolae and less prominent giant rugae than giant rugai hypertrophy.
Secondly, giant rugae as seen in Fig.6"-11 were composed of foveolar elongation of fundic mucosa in stomal poiypoid hypertrophic gastritis and CronkhiteCanada syndrome. The giant rugae in the former arised from gastric mucosa just near the gastroenteric stoma and therefrom extended along mucosal folds within the area less than four centimeters. They showed hyperplasia of generally immature foveolar epithelium, beneath which a marked increase in number and size of pseudopyloric glands and atrophy of fundic glands were seen. Giant rugae in Cronkhite-Canada syndrome were usually made up of union of sessile polyps which were distributed in the antrurn as well. They indicated hyperplasia of mature, hypersecretory foveolar cells, and dilatation of foveolar tubules with subsequent cyst formation.
Thirdly, giant rugae as seen in Fig.3~5 were formed of an increase in number of pseudopyloric glands and their cysts in the normal thickness of fundic mucosa.
Fourthly, giant rugae as seen in Fig.18~21 were made up of tumor tissues (malignant lymphoma, benign lymphoicl hyperplasia, carcinoma, etc.) in the mucosa and/or subrnucosa, and they consisted of widening of lamina propria in acute gastritis.
Sixthly, giant rugae as seen in Fig.12~17 were formed of submucosal thickening, redundancy of mucosa, passive elongation of mucosa and simple hyperplasia of fundic mucosa with a very mild degree of pseudopyloric glands and their microcysts, or without any such change. They were typical of carcinoma of linitis plastica type. However, most of the giant rugae were mainly formed of the former two histologic findings described above.
Seventhly, giant rugae were composed of only subrnucosal factor: inflammation, fibrosis or tumors.
Each gastric disease with giant rugae histologically has characteristic features. Therefore, we can differentiate them prior operation by endoscopic biopsy with the help of x-ray and endoscopic findings of the lesions. It will be fruitful in study on early detection, prospective changes in morphology, and function of giant rugal diseases in unknown as well as known nature.
Copyright © 1980, Igaku-Shoin Ltd. All rights reserved.

