Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
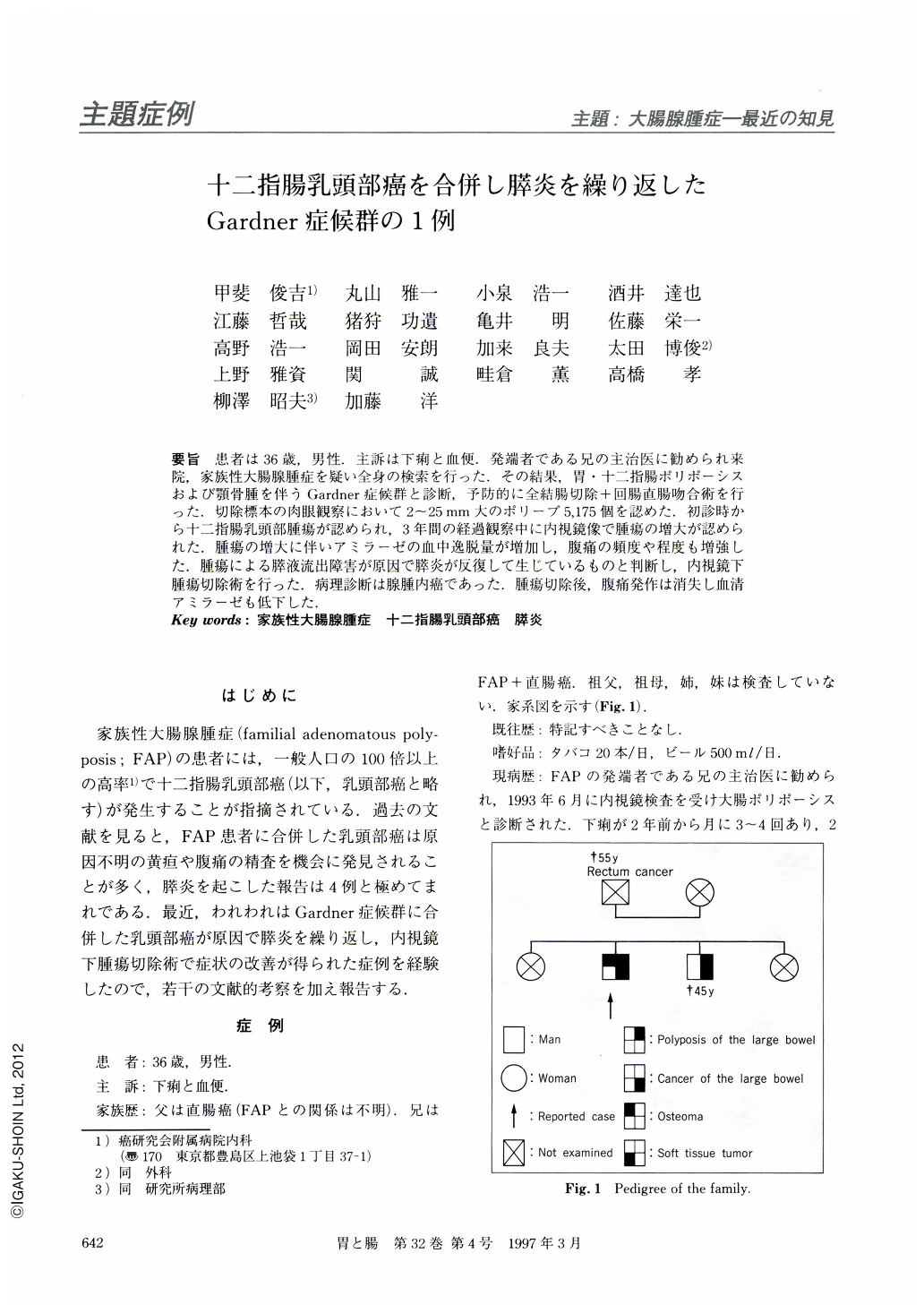
要旨 患者は36歳,男性.主訴は下痢と血便.発端者である兄の主治医に勧められ来院,家族性大腸腺腫症を疑い全身の検索を行った.その結果,胃・十二指腸ポリポーシスおよび顎骨腫を伴うGardner症候群と診断,予防的に全結腸切除+回腸直腸吻合術を行った.切除標本の肉眼観察において2~25mm大のポリープ5,175個を認めた.初診時から十二指腸乳頭部腫瘍が認められ,3年間の経過観察中に内視鏡像で腫瘍の増大が認められた.腫瘍の増大に伴いアミラーゼの血中逸脱量が増加し,腹痛の頻度や程度も増強した.腫瘍による膵液流出障害が原因で膵炎が反復して生じているものと判断し,内視鏡下腫瘍切除術を行った.病理診断は腺腫内癌であった.腫瘍切除後,腹痛発作は消失し血清アミラーゼも低下した.
A 36-year-old man visited our institution with complaints of bloody stool and diarrhea. In July 1993, he was found to have numerous colonic adenomas, duodenal papilla adenoma and osteomas of mandibula, and was diagnosed with Gardner's syndrome (Fig. 2). In September 1993, the patient underwent a total colectomy with ileorectal anastomosis. The resected specimen showed as many as 5,157 polypoid lesions throughout the colon (Fig. 3). Follow-up examination revealed increase of the duodenal papilla in size for the 30 months, but malignant transformation was not detected at the time of endoscopic biopsy. Recurrent pancreatitis was thought to be caused by the obstruction of the pacreatic duct due to the enlarged duodenal papilla. Therefore the patient underwent endoscopic papillectomy in July 1996. Recurrent pancreatitis has disappeared since the procedure. The pathological diagnosis of the polypectomized specimen was a tubular adenoma with minute cancer which was limited within the mucosa (Fig. 6). Once invasive cancer of the duodenal papilla has developed, high mortality rate is expected. Therefore, it is important to repeat follow-up endoscopic examinations with biopsy for duodenal papilla adenoma. If it is resectable, endoscopic treatment may be recommended in its early stage.
Copyright © 1997, Igaku-Shoin Ltd. All rights reserved.

