Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
モヤモヤ病の成因はいまだ不明であるが,脳血管撮影で両側内頸動脈終末部の進行性閉塞性病変と脳底部の異常血管網を示すものが確診例と診断され,一側性病変のみをしめすものは疑診例とされている6).モヤモヤ病の成人例において一側性病変から両側性病変への進行は極めて稀であるとされ,その経過が確認された報告例も少ない1,7,14).今回われわれはモヤモヤ病成人例において,発症後4年間で一側性の閉塞性病変が両側性病変へ進行し,急速な悪化を示し死亡に至った1例を経験したので,文献的考察を加え報告する.
We reported a case of adult moyamoya disease show-ing acute deterioration in which a unilateral occlusive lesion progressed to bilateral involvement during a period of 49 months.
A 54-year-old male suffered from progressive weak-ness in his right extremities and disturbance of speech. On admission, neurological examination demonstrated mild right hemiparesis with global aphasia.
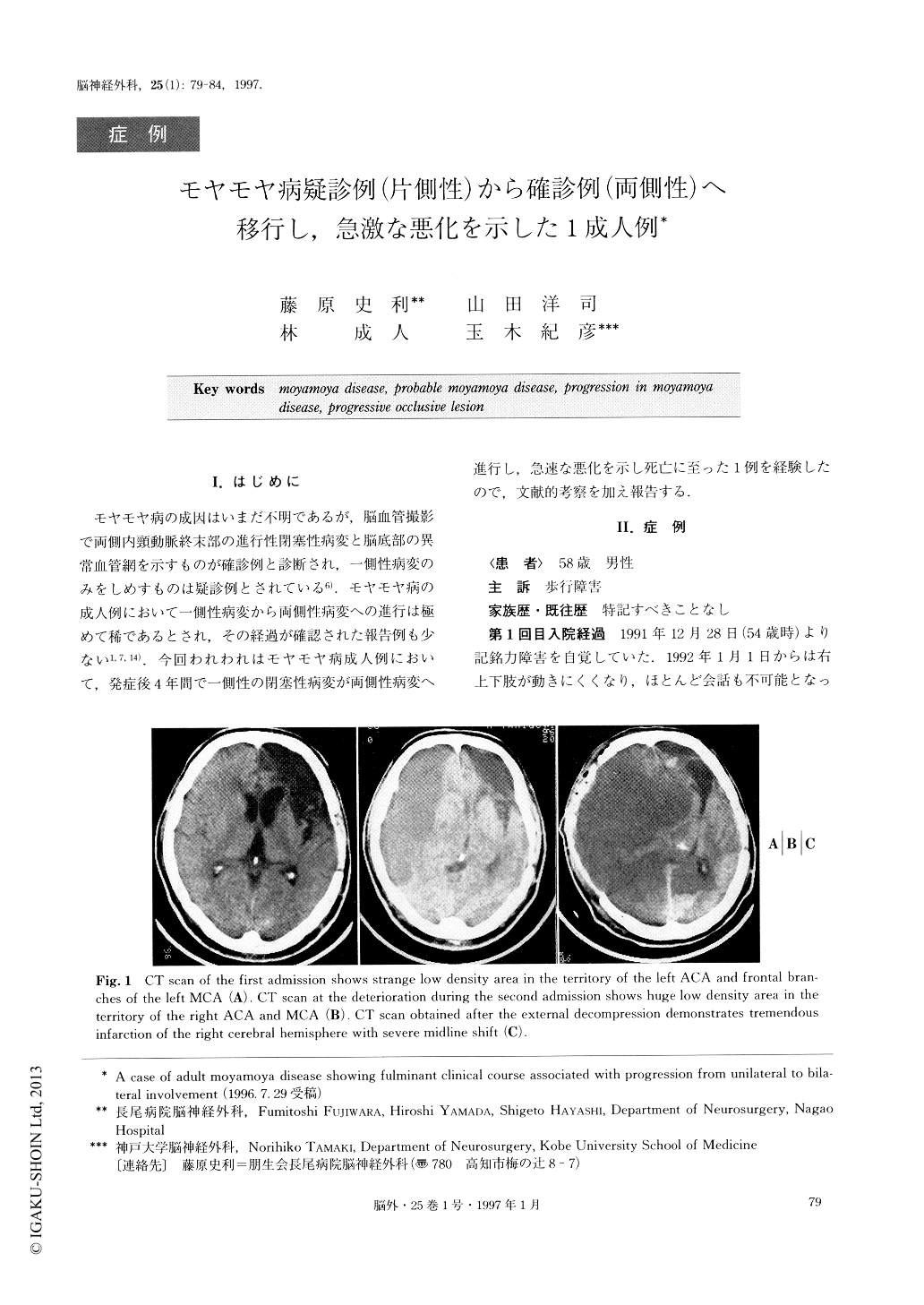
A computed tomography (CT) scan showed a strange low density area in the territory of the left ACA and frontal branches of the left MCA. Left caro-tid angiography showed stenosis of the ICA at the ter-minal portion, occlusion of the ACA and MCA at each origin, and basal moyamoya vessels. Right carotid an-giography demonstrated no occlusive lesions except for the general narrowing of the right ACA, without moya-moya vessels.
This case was classified as adult-onset “probable” moyamoya disease according to the diagnostic criteria of the Japan Cooperative Research Committee. Left su-perficial temporal artery-middle cerebral artery (STA-MCA) anastomosis was performed. The patient showed gradual amelioration of neurological symptoms, and was discharged on foot with mild motor aphasia. However, 4 years later he complained of weakness inhis left lower extremitiy. A second cerebral angiogra-phy, performed 49 months after the initial angiography demonstrated severe stenosis of the left ICA at the ter-minal portion progressing in the proximal direction with decreasing basal moyamoya vessels, while severe stenosis extended from the terminal portion of the right ICA to the Ml portion with newly developed moyamoya vessels in the right basal area. At this time, we considered that this case was a definite case of moyamoya disease. The second cerebral angiography was completed uneventfully. However, the patient then suddenly showed acute deterioration 5 hours after the angiography. Emergent cerebral angiography disclosed an occlusion of the right ICA at the terminal portion. Thereafter he showed acute deterioration in conscious-ness. A CT scan at the time revealed a huge low densi-ty area in the territory of the right ACA and MCA. We performed emergent external decompresion, but he did not recover from the sequelae of cerebral infarction and died 3 days later.
This rare case suggested the possibility of progres-sion to bilateral involvement although it was a case of adult-onset “probable” moyamoya disease. We consider that acute ischemic deterioration should be kept in mind especially in aged cases of adult-onset moyamoya disease. Careful observation should be performed by the serial MR angiography in adults with “probable” moyamoya disease even though they are clinically asymptomatic.
Copyright © 1997, Igaku-Shoin Ltd. All rights reserved.

