Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
脳膿瘍の治療法については,議論の別れるところであるが,一般には,急性炎症がおさまり,被膜が形成される時期に膿汁の穿刺吸引が行われる.そして数回の穿刺排膿を繰り返しても脳膿瘍が完全に退縮しない場合や,短期間に再貯留する場合には,被膜外摘出術が行われている.しかし従来行われてきたような用手的な穿刺法では,1回の穿刺で正確に膿瘍に的中させて,十分な排膿を行うことが困難な場合が少なからずある.
そこで今回著者らは,主に深在性の脳膿瘍に対し,CT誘導による定位的吸引術を行ったので,手術成績および術後経過などについて報告する.
Abstract
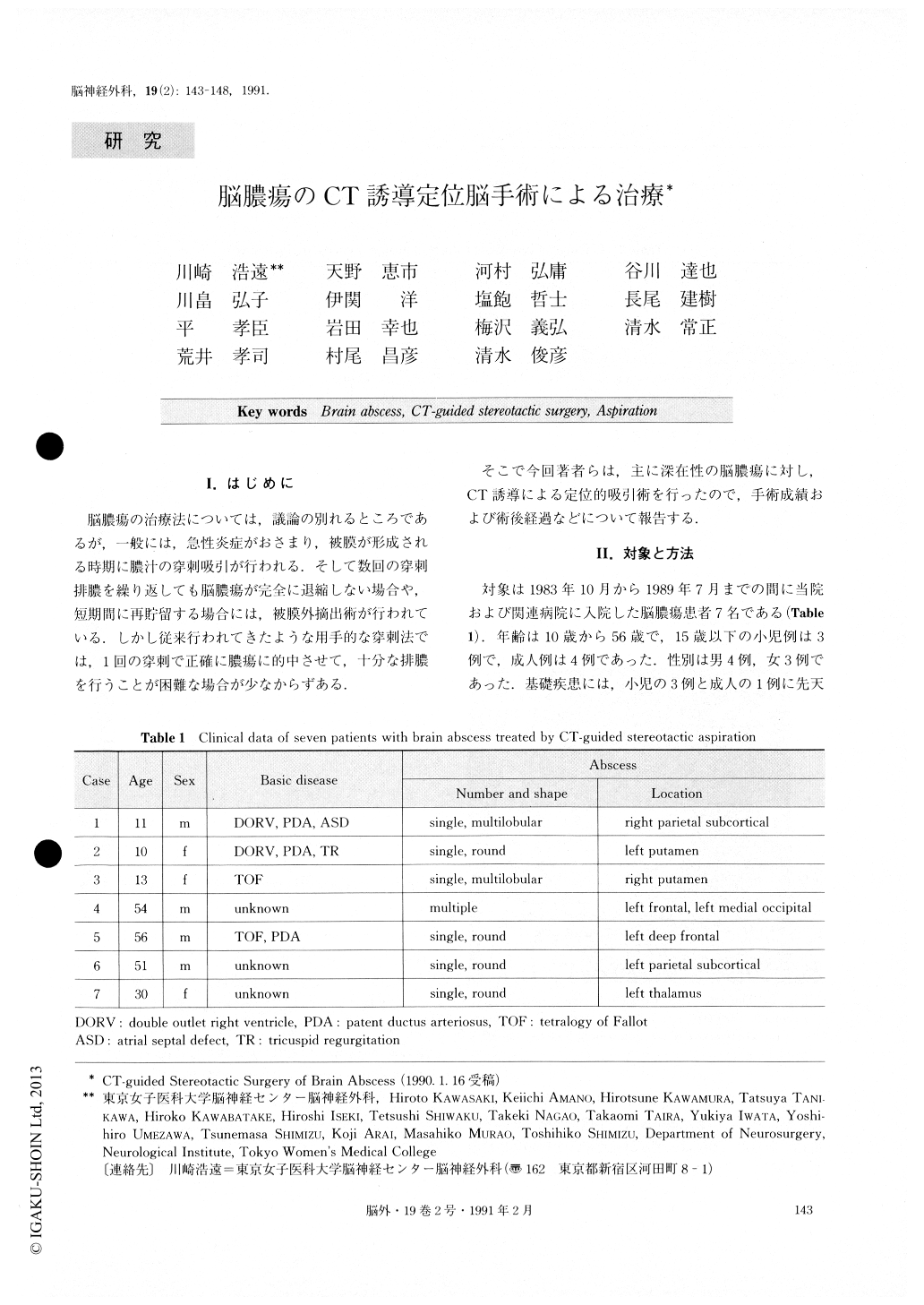
Seven patients with brain abscess underwent CT-guided stereotactic aspiration using Iseki's stereotactic apparatus. Three of them were under the age of fifteen and four were older than thirty. The lesions were single and round in four cases, multilobular in two and multi-ple in one patient.
Operations were performed after systemic adminis-tration of antibiotics for more than two weeks and after capsule formation was confirmed on CTs. Preoperative volume of the abscesses was estimated from CTs. The target point chosen was the center of the ring of the largest diameter in the enhanced lesion. Abscess was aspirated under monitoring with intraoperative CT scan. No continuous drainage was performed and no antibiotics were given directly into the abscess cavity. In all cases the center of the abscess was punctured with a single trial. Average volume of the preoperative brain abscesses was 18.8ml. Aspirated volume at the time of the operation averaged 16.9m1 and all the abscesses decreased to unmeasurable size on CTs. In five of seven patients abscesses were cured after a sing-le aspiration, and in one case after the second opera-tion. One case required extirpation of the lesion. During the follow-up period of four months to five and a half years six patients showed no recurrence. One patient died of unrelated cause four and a half years after the operation. No operative complication was noted. There was no operative morbidity or mortality.
Using a CT guided stereotactic method, brain abs-cess is punctured so accurately, regardless of its loca-tion and size, that damage to the surrounding brain during operation can be minimized. Therefore it is highly possible to aspirate abscesses completely. Opera-tive complication such as bleeding into an abscess cav-ity is unlikely because of intraoperative monitoring with CT scan, which is one of the major advantages of Iseki's stereotactic apparatus. If the abscess is com-pletely aspirated, the authors believe that direct admi-nistration of antibiotics into an abscess cavity, or post-operative drainage is unnecessary.
In conclusion, CT-guided stereotactic aspiration is the treatment of first choice for brain abscess especially when it is small or deep seated. This method is consi-dered to be superior to the conventional free-hand aspiration even if ultrasound guidance is employed, be-cause of the higher resolution of the CT scan and pre-cise targeting.
Copyright © 1991, Igaku-Shoin Ltd. All rights reserved.

