Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
特発性の片側顔面痙攣の治療は,顔面神経の起始部,いわゆるexit zoneでの圧迫血管(offending vessel)を移動させ,これによる神経圧迫を除く手術がGardnerら5)により試みられ,Jannettaらによりmicrovascular de—compression(以下MVDと略)として確立6)されて以来,近年盛んに行われ成果をあげている.
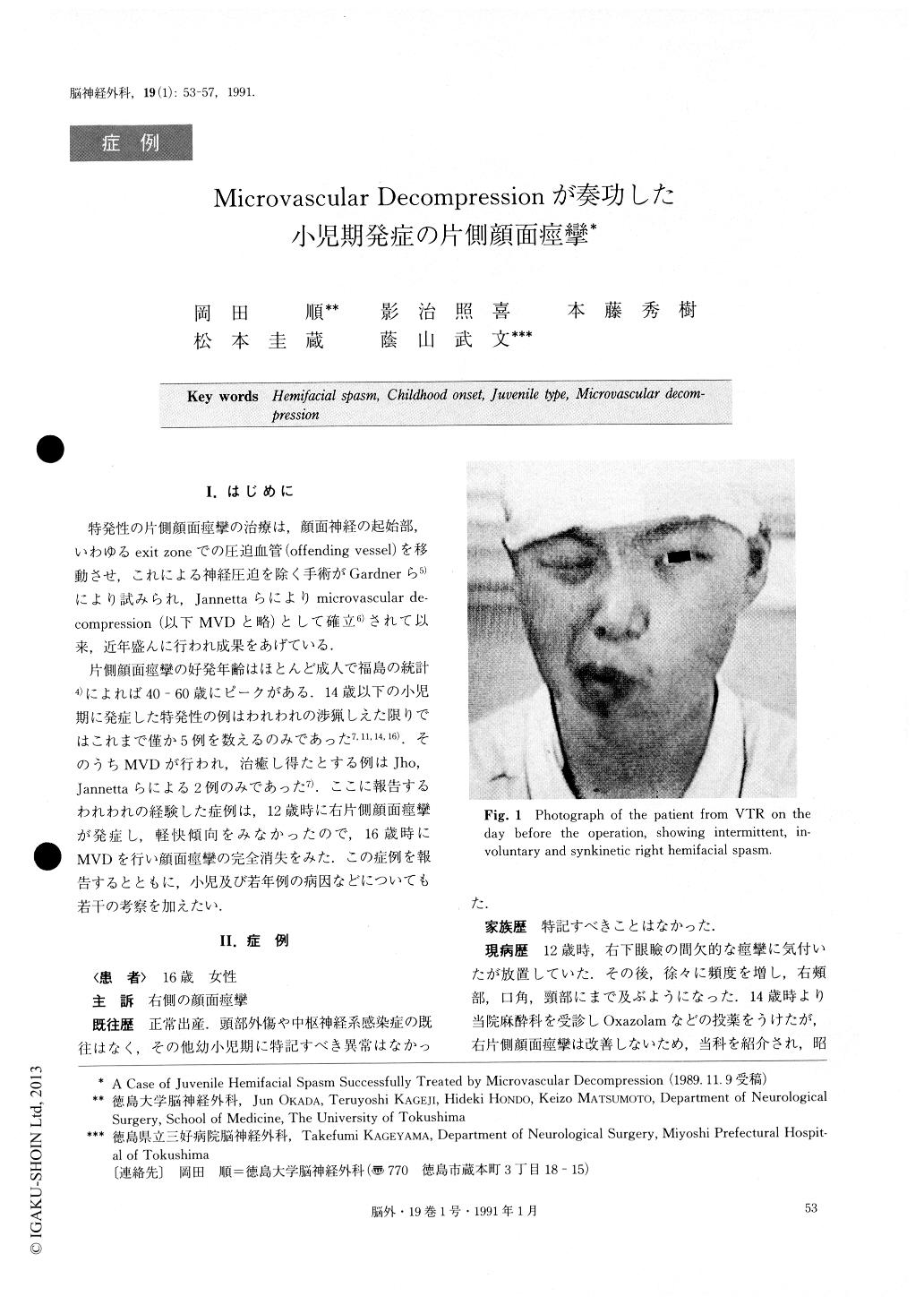
片側顔面痙攣の好発年齢はほとんど成人で福島の統計4)によれば40-60歳にピークがある.14歳以下の小児期に発症した特発性の例はわれわれの渉猟しえた限りではこれまで僅か5例を数えるのみであった7,11,14,16).そのうちMVDが行われ,治癒し得たとする例はJho,Jannettaらによる2例のみであった7).ここに報告するわれわれの経験した症例は,12歳時に右片側顔面痙攣が発症し,軽快傾向をみなかったので,16歳時にMVDを行い顔面痙攣の完全消失をみた。この症例を報告するとともに,小児及び若年例の病因などについても若干の考察を加えたい.
A 16-year-old girl had an episode of intermittent in-voluntary spasm of the right inferior orbicularis oculi muscle at the age of 12. In the following years the right orbicularis oris muscle and platysma were unilaterally and progressively involved in the spasms and with in-creasing frequency. Medical treatment with minor tran-quilizer was not effective.
She was referred to our department at the age of 16. CT and MRI revealed no abnormality. Angiographical study revealed that the right PICA (posterior inferior cerebellar artery) was tourtously coming off from a re-latively high portion of the right vertebral artery. The trunk of the right AICA (anterior inferior cerebellar artery) was not able to be identified.
Although the onset of this condition was unusually early, the clinical course and symptoms of hemifacial spasm were so clearly typical that she underwent mi-crovascular decompression surgery on July 26, 1988, at the age of 16.
During the operation an upward looping PICA was found crossing and tightly compressing the exit zone of the right facial nerve. The offending artery seemed to be elastic without significant atherosclerotic change. The arterial loop was carefully dissected and replacedwith two pieces of sponge prosthesis between the artery and the surface of brain stem.
Her hemifacial spasm completely disappeared post-operatively. No recurrence has been noted for over one year in the follw-up observation.
Hemifacial spasm is subacutely or chronically a pro-gressive disorder of facial involuntary movement. The arterial compression in the exit zone of the facial nerve is said to be the cause of the disorder and microvascu-lar decompression has been indicated for it since a little before the beginning of this decade. Hemifacial spasm is considerably frequent in middle or more advanced ages. In such patients the offending artery often shows atherosclerotic changes which may be one of the re-sponsible factors for the arterial compression. Although juvenile cases of hemifacial spasm are very rare, in the literature a few cases of children who underwent opera-tion are reported. In those unusually young cases in-cluding our case, during the operation, no expressive atherosclerotic change seemed to be shown. The lack of atherosclerotic arterial elongation may explain the rare incidence of hemifacial spasm in childhood. However normal variations in AICA and PICA are numerous even in young persons, and they may cause the arterial compression in the exit zone of the facial nerve without atherosclerotic change.
Hemifacial spasm in childhood must be differentiated from other disorders, especially from facial tic. If it is differentiated with its characteristic symptoms, and if it is severe enough to disable the young patient psycholo-gically or socially, microvascular decompression should be the treatment of choice.
A successful case of microvascular decompression for juvenile hemifacial spasm is reported.
Copyright © 1991, Igaku-Shoin Ltd. All rights reserved.

