Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
はじめに
くも膜下出血症例に対しては,積極的に出血源の所在を探究し,それに対して適切な治療を加える方向が主流を占めつつある。近時脳動脈瘤,動静脈奇型等に対する外科的根治療法の進歩と普及により,この方面での治療成績の向上にはめざましいものがある。
ここで問題となるのは,脳血管撮影によつても出血源を証明することができず,しかも出血の原因となるような疾患も臨床上認められない症例である。これら症例では,臨床像は立派なくも膜下出血であるにも拘らず,治療の面からみて不徹底の感を免れない。またどのような要因によつて起るのか,どのような運命を辿るものか,についても従来検討に乏しいことが痛感される。
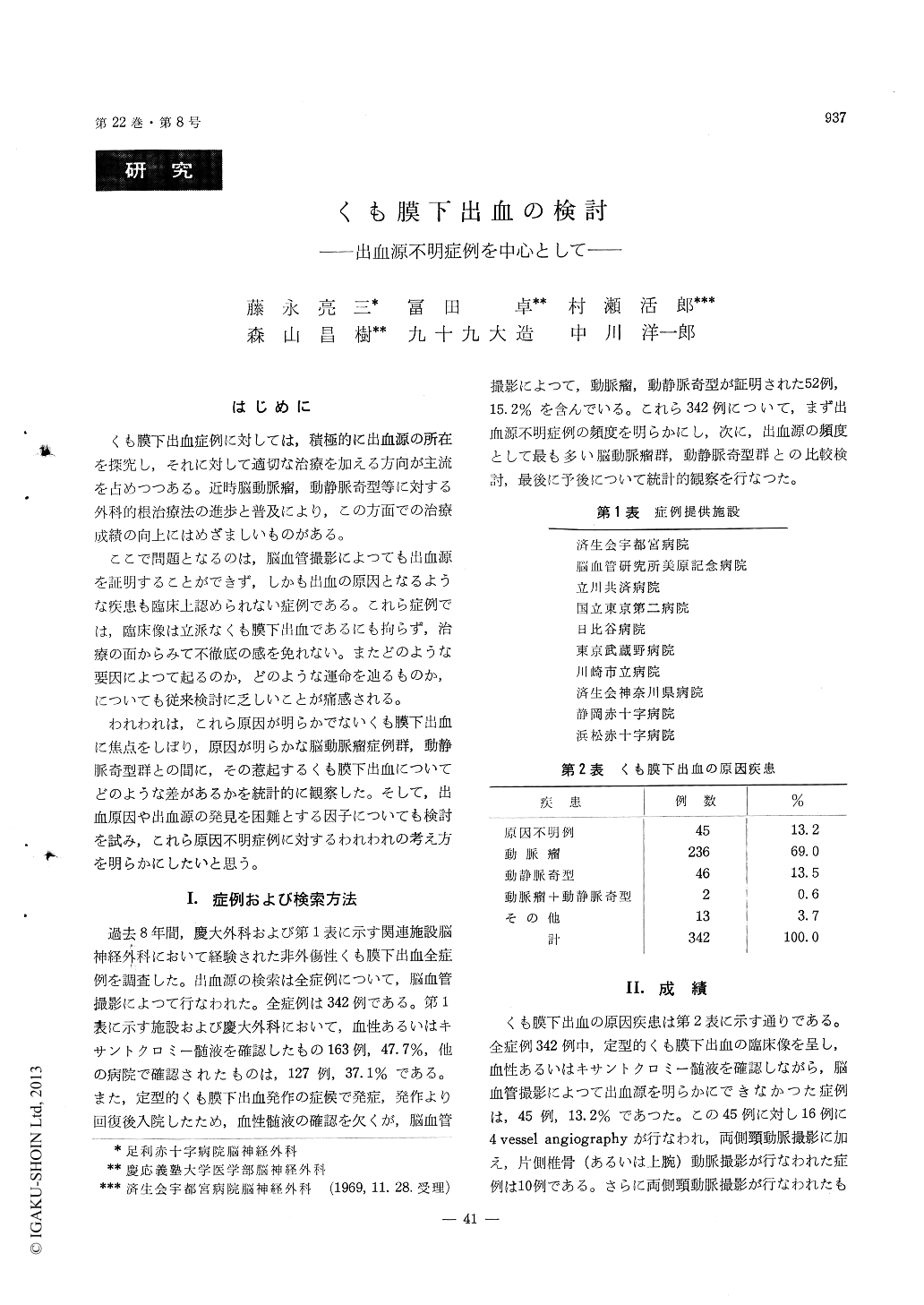
Out of 342 cases of clinically diagnosed SAH between 1961 and 1968 from Keio University Hos-pital and other 10 cooperative institutes, forty-five cases (13. 2%) are screened out in this series in which the cause of bleeding can not be identified by repeated angiography and other examinations.
By detailed analysis of these unidentified cases, the characteristics are lined up as follow in com-parison with the cases of verified aneurysm and A-V malformation.
1. Age distribution has two peaks namely in 30-40 and 50-60 years of age whereas the a neurysm in 30-60 and A-V malformation in 10-30 years of age.
2. The episode of SAH is milder in manifesta-tion and less in the frequency of the recurrence.
3. C. S. F. is more rapidly cleared up.
4. The post-episodic sequella is less and severe neurological deficiencies remain rarely even thoughthe initial attack manifests typical SAH.
5. Prognosis is benign and mortality rate is only 2. 6% whereas 25. 8% in aneurysm and 10% in A-V malformation. All cases of SAH of unidentified etiology in this series evaluated by 4 vessel angio-graphy survive and return to the previous pro-fession except one.
Other multiple estimated etiologies were proposed by Locksley (1966) however there is no analogous case in our series except for 6 hypertensive intra-cerebral hemorrhage, 2 arterial thrembosis and 1 thrombocytopenic purpura as basic disease. The most possible cause of the unidentified SAH is thought to be the rupture of hidden micro-aneurysm on angiogram exceeding the level of usual angio-graphical analysis as pointed out by Krayenbuhl or due to the spontaneous thrombus formation in the ruptured aneurysm. As for the latter, we experien-ced 4 × 4 × 3 mm berry type aneurysm disappeared completely in the course of hospitalization which was clearly demonstrated on repeated angiography.
In addition, we succeeded in verifying the ru-ptured micropial vessel causing thin hemorrhage in the subarachnoidal space due to angionecrosis terminated by the rupture of the another coexisting berry type aneurysm. This also indicates the possi-bility of such instance in case of the aged group with hypertensive arteriosclerotic vascular changes.
Copyright © 1970, Igaku-Shoin Ltd. All rights reserved.

