Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
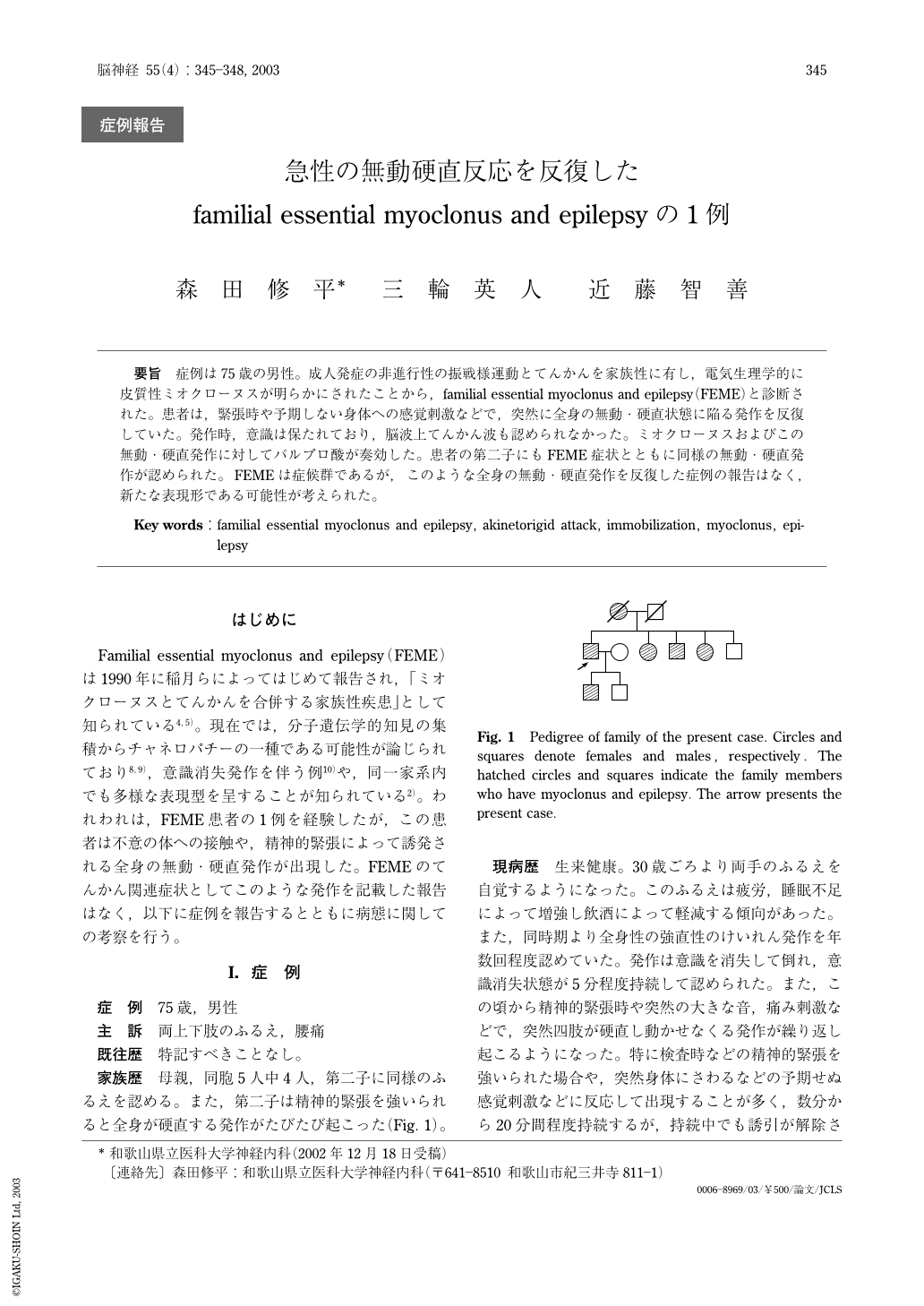
要旨 症例は75歳の男性。成人発症の非進行性の振戦様運動とてんかんを家族性に有し,電気生理学的に皮質性ミオクローヌスが明らかにされたことから,familial essential myoclonus and epilepsy(FEME)と診断された。患者は,緊張時や予期しない身体への感覚刺激などで,突然に全身の無動・硬直状態に陥る発作を反復していた。発作時,意識は保たれており,脳波上てんかん波も認められなかった。ミオクローヌスおよびこの無動・硬直発作に対してバルプロ酸が奏効した。患者の第二子にもFEME症状とともに同様の無動・硬直発作が認められた。FEMEは症候群であるが,このような全身の無動・硬直発作を反復した症例の報告はなく,新たな表現形である可能性が考えられた。
A 75-year-old Japanese man who had a past history of epilepsy was admitted because of rhythmical myoclonus of upper and lower extremities. His mother and son also had both epilepsy and myoclonus. On neurological examination, he was alert and oriented without dementia. There was no abnormal finding except for the myoclonic jerks appearing in his upper and lower extremities. The myoclonic jerks appeared at rest and worsened during maintaining posture. Results of laboratory tests were all within normal levels. Brain MRIs were normal, and his EEGs showed diffuse fast wave activities without paroxysmal discharges. Surface EMG studies revealed irregular myoclonic discharges at the frequency of 6-20Hz. Electrophysiologically, he had a giant somatosensory-evoked potentials, an enhanced long-loop reflex(C-reflex) and cortical spikes preceding the myoclonic jerks, suggesting that his myoclonus was of cortical origin. Based on the cortical myoclonus, episodes of epilepsy and familiarity, he was diagnosed as having familial essential myoclonus and epilepsy(FEME). In addition, he periodically became a motionless state characterized by sudden appearance of transient akinesia with generalized stiffness of all of his limbs. The transient motionless state usually appeared following mental stress or sudden sensory stimuli such as loud sound. It persisted for about 10-20min and ceased spontaneously. Since EEGs recorded during this akinetorigid state showed no paroxysmal discharges, it was considered not to be epileptic. However, after the administration of valproate, his cortical myoclonus improved, and the transient akinetorigid state also disappeared simultaneously. From symptomatic point of views, this generalized motionless state with stiffness of limbs may resemble to freeze behavior of wild animals suddenly confronted with sudden strong stimuli. From symptomatological as well as genetic aspects, FEME has been suggested to be heterogeneous. We propose that this unique akinetorigid attack might be a new clinical phenotype of FEME.
Copyright © 2003, Igaku-Shoin Ltd. All rights reserved.

