Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
緒言
脳動脈瘤の直接手術に際していかなる麻酔が最も安全であるか,特に常温下全身麻酔と低体温麻酔とのいずれが優れているかについては今日なお討論のあるところである3)8)11)。一般に低体温麻酔の利点としては脳血流遮断時間の延長,dry field下手術,脳容積の縮小などがあり,欠点としては循環器系合併症特に心室細動が起こり易いこと,手技が繁雑であることなどである。こうしたメリットとデメリットとをバランスシートにかけて,どちらがより大きいかで低体温麻酔の是非がきまるわけである。
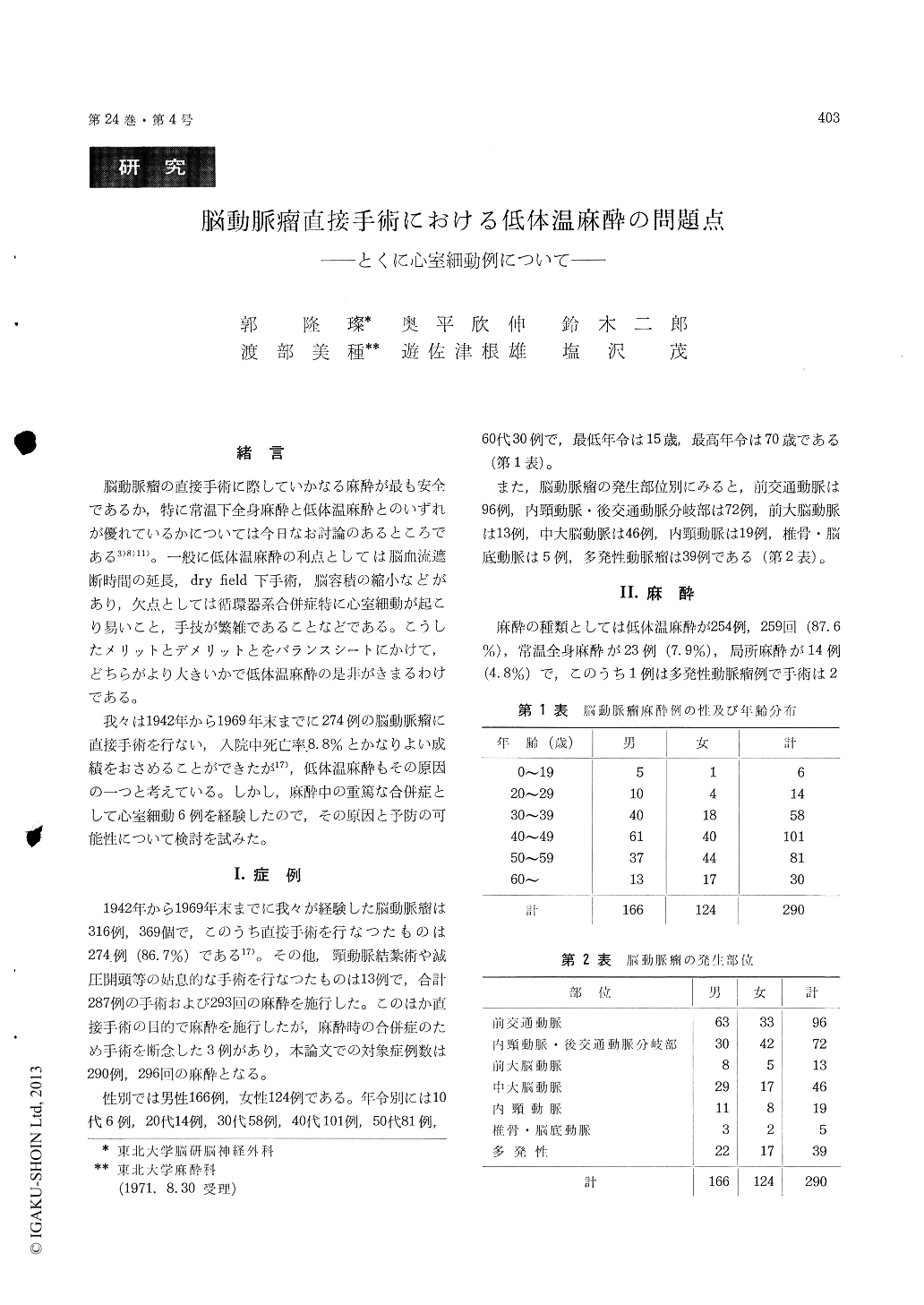
我々は1942年から1969年末までに274例の脳動脈瘤に直接手術を行ない,入院中死亡率8.8%とかなりよい成績をおさめることができたが17),低体温麻酔もその原因の一つと考えている。しかし,麻酔中の重篤な合併症として心室細動6例を経験したので,その原因と予防の可能性について検討を試みた。
The direct surgical treatment of intracranial aneurysms was performed in 274 cases in our in-stitute from 1942 up to the end of 1969.
Mortality rate during hospitalization was 8. 8 per cent. Hypothermic anesthesia seemed to be one of the factors attributed to this low rate of mortality. On the other hand, ventricular fibrillation was the most serious complication in hypothermic anesthesia.
Problems in hypothermic anesthesia for direct surgical treatment of intracranial aneurysms were discussed, with special reference to ventricular fibrillation.
1. Direct surgical treatments were performed in251 cases among 254 cases of intracranial aneurysmsunder hypothermic anesthesia in 259 times. Inthree cases the operation had to be cancelled dueto the occurrence of ventricular fibrillation.
2. During hypothermia ether was used in 95.4per cent, while fluothane in 3.0 per cent and pen-thrane in 1.7 per cent.
3. Moderate hypothermic anesthesia was per-formed in almost all cases (90 per cent), with thelowest body temperature ranging between 25-29℃.
4. Complications occurred in 61 cases (24 percent), but most of them were transient arrhythmiasand did not affect the postoperative course exceptventricular fibrillation.
5. Ventricular fibrillation occurred in 6 cases (2.4 per cent). Five cases were successfully resusci-tated, three cases of which were operated unevent-fully, but two cases had to be cancelled in perform-ing surgery and one case could not be resuscitated.
6. The possible causes of ventricular fibrillationin these cases were thought to be postural changes,especially an abrupt change of the head and neckposition, decrease in effective circulatory bloodvolume due to mannitol transfusion added for pre-operative dehydration, hypersensitivity of the heartunder fluothane anesthesia as well as ventricularhypertrophy or myocardial damage.
Copyright © 1972, Igaku-Shoin Ltd. All rights reserved.

