Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
- サイト内被引用 Cited by
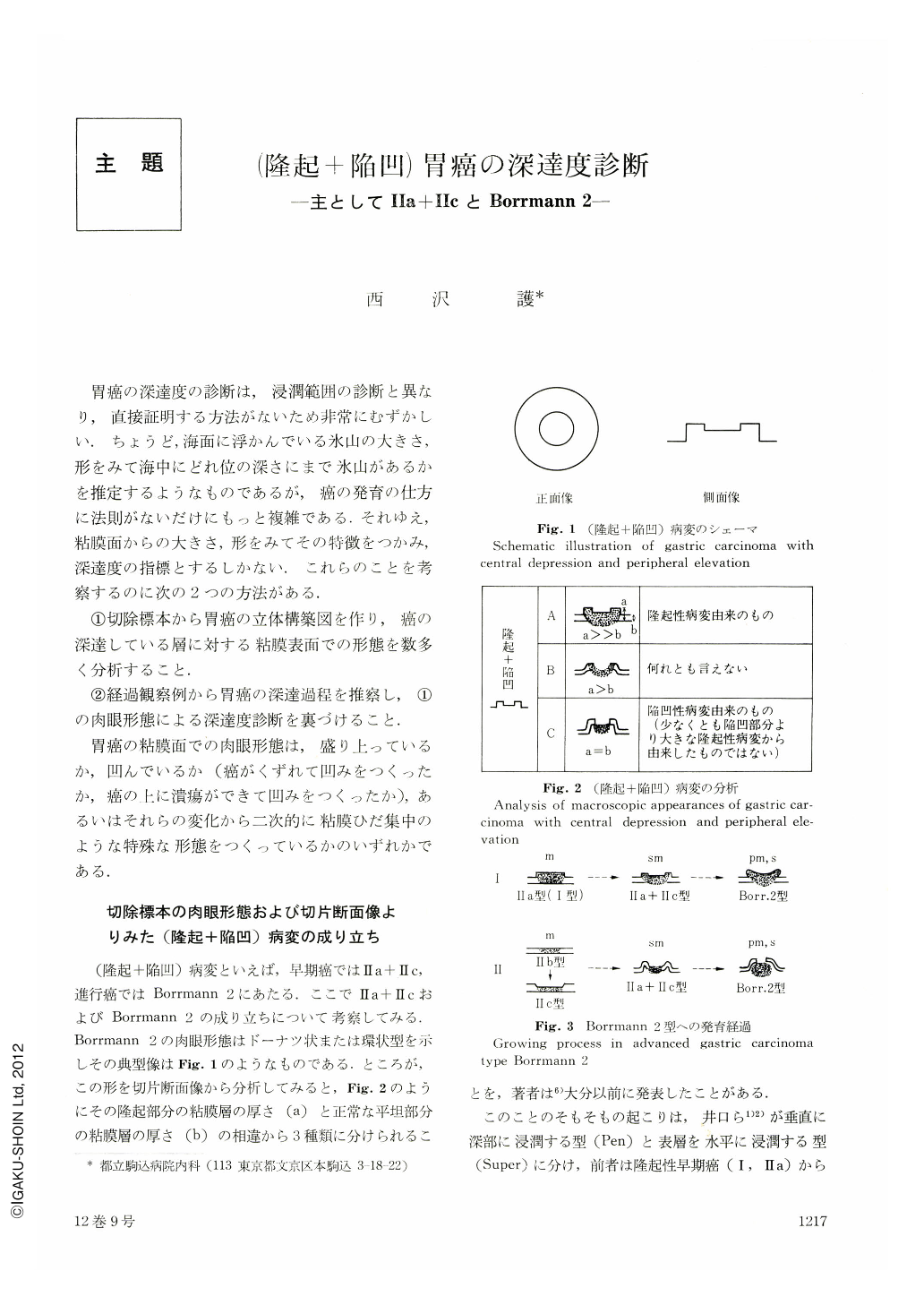
胃癌の深達度の診断は,浸潤範囲の診断と異なり,直接証明する方法がないため非常にむずかしい.ちょうど,海面に浮かんでいる氷山の大きさ,形をみて海中にどれ位の深さにまで氷山があるかを推定するようなものであるが,癌の発育の仕方に法則がないだけにもっと複雑である.それゆえ,粘膜面からの大きさ,形をみてその特徴をつかみ,深達度の指標とするしかない.これらのことを考察するのに次の2つの方法がある.
①切除標本から胃癌の立体構築図を作り,癌の深達している層に対する粘膜表面での形態を数多く分析すること.
②経過観察例から胃癌の深達過程を推察し,①の肉眼形態による深達度診断を裏づけること.
胃癌の粘膜面でめ肉眼形態は,盛り上っているか,凹んでいるか(癌がくずれて凹みをつくったか,癌の上に潰瘍ができて凹みをつくったか),あるいはそれらの変化から二次的に粘膜ひだ集中のような特殊な形態をつくっているかのいずれかである.
For pre-operative estimation of the depth of invasion in gastric carcinoma, it is important to see how gastric wall looks like on barium filled view in barium meal study. Conventional X-ray findings such as filling defect and rigidity of the gastric wall are still considered as the most indicative signs to presume the depth of invasion. However, if carcinoma does not lie across either of the curvatures, diagnostic signs are hardly seen on the barium filled view of the stomach. Therefore, diagnostic information displayed on the front view of the carcinoma should be analyzed to know how deep the invasion reaches.
Generally speaking, the depth of invasion in gastric carcionma seemed to be accurately diagnosed in 80~90% of cases, although the results altered according to the proportion of early carcinoma to advanced carcinoma.
It is not so easy to assess pre-operatively to which layer of the gastric wall invation of carcinoma goes down.
In this paper, X-ray and endoscopic findings of gastric carcinomas with central depression and peripheral elevation as well as their macroscopic and microscopic appearances are analyzed to search for diagnostic signs suggestive of the depth of invasion and the results are as follows.
1. Both protrude (type Ⅰ and Ⅱa) and depressed types of early gastric carcinoma may grow up to advanced carcinoma type Borrmann 2 and more advanced carcinomas type Borrmann 2 seem to originate from depressed type early gastric carcinoma.
In gastric carcinoma of this type developed from depressed early gastric carcinoma, invasion came down to deeper layer of the stomach than in those developed from protruded early gastric carcinoma in the same size.
2. Most of gastric carcinomas with central depression and peripheral elevation less than 20 mm in diameter were early carcinoma and the majority of gastric carcinomas of this type more than 40 mm in diameter were advanced carcinoma. There were a few cases of early carcinoma of this type more than 40 mm in diameter and all had submucosal invasion.
3. Macroscopic appearances of this type gastric carcinoma with central depression and peripheral elevation were different between those developed from depressed type early gastric carcinoma and protruded early gastric carcinoma. The characteristic macroscopic appearances of gastric carcinoma of this type developed from elevated gastric carcinoma were irregular margin and rough granular surface of the tumor without mucosal folds convergence. The foot of the tumor was steep-sloped or looked like having waist. On the other hand, there were two separate types of gastric carcinoma with an original shape of mucosal depression, one with convergence of mucosal folds and the other without mucosal folds convergence. Clubbing and fusion of the mucosal folds were seen in the former type and occasionally converging mucosal folds looked like bridgingfolds. The surface of the tumor appeared smooth and the tumor was rather regularly outlined in this type of gastric carcinoma developed from depressed early gastric carcinoma. There was no infiltration of carcinoma in the periphery of the tumor. The foot was gently sloped.
4. Thus, original shape of these carcinomas with central depression and peripheral elevation may be assumed by demonstrating faithfully the macroscopic and microscopic appearances of these carcinomas using X-ray and gastroscopy with biopsy.
5. Gastric carcinomas of this type with an original form of mucosal protrusion less than 30 mm in diameter were early carcinoma and those more than 30 mm in diameter were advanced carcinoma. In the same size of carcinoma, the deeper and bigger central depression was, the deeper invasion reached.
6. Submucosal invasion was always seen in the gastric carcinoma of this type with an original form of mucosal depression less than 20 mm in diameter and in those more than 20 mm in diameter were advanced carcinoma. In the same size of the carcinoma of this type, the depth of invasion seemed to be proportionate to the height of peripheral protrusion of the tumor and the depth of central depression.
Copyright © 1977, Igaku-Shoin Ltd. All rights reserved.

