Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
- 参考文献 Reference
Stanford A型急性大動脈解離における臓器灌流障害(malperfusion)は予後不良因子であり,罹患臓器と発生機序に応じた迅速な処置が重要である.近年,static obstructionの症例に対してcentral repairより先に虚血臓器の灌流を優先させることで,治療成績の改善が期待されている1).当科での成績を報告する.
Background:For malperfusion in Stanford type A acute aortic dissection, we resolve static intestinal ischemia prior to central repair, rapidly unload the left ventricle for myocardial ischemia, and resolve cerebral or lower limb ischemia using cardiopulmonary bypass. We evaluated the validity of this strategy.
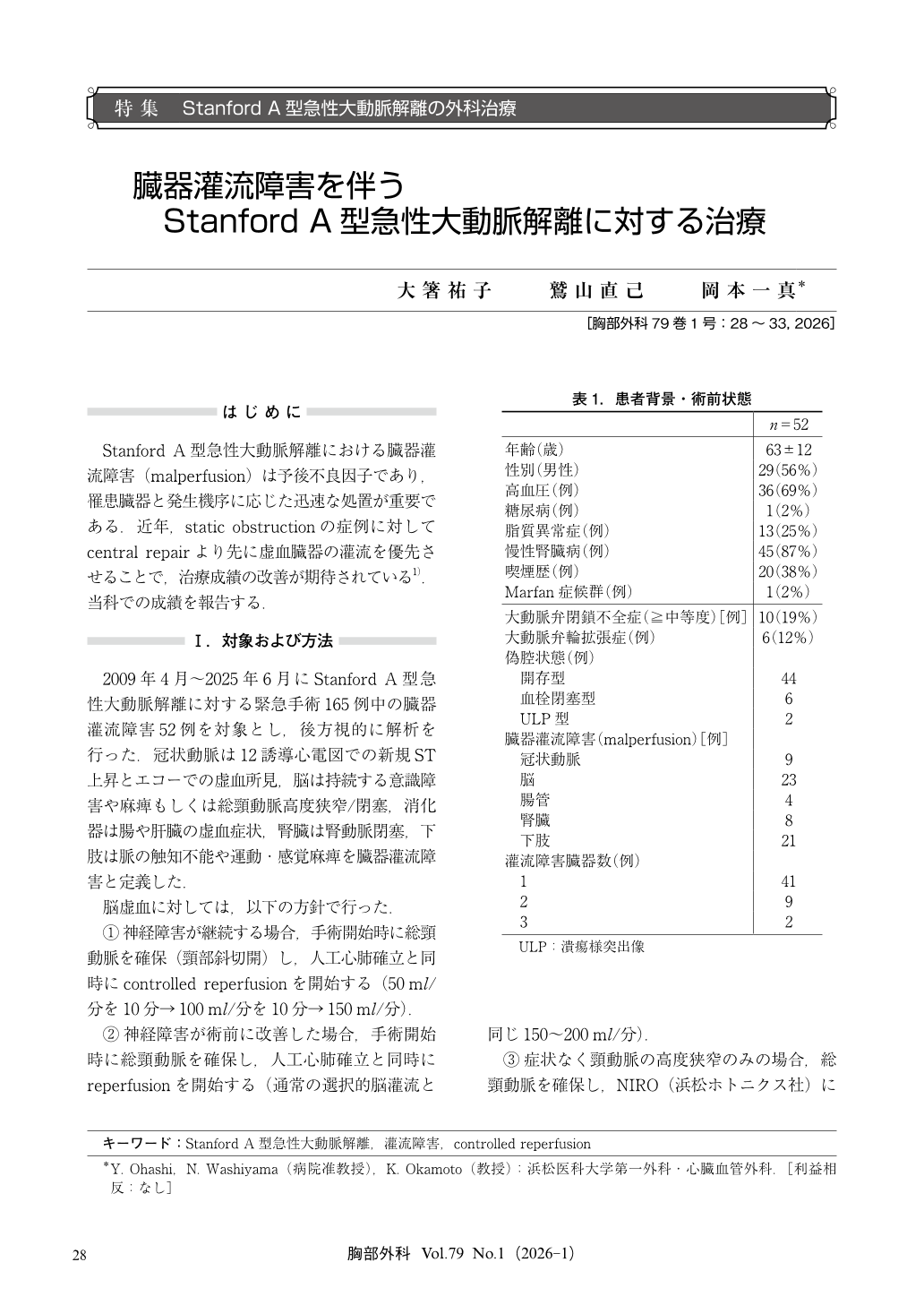
Subjects:Among 165 emergency surgeries for Stanford type A acute aortic dissection performed since 2009, malperfusion was present in 52 cases (brain 23/heart 9/kidney 8/intestine 4/lower extremity 21)[overlap present].
Results:Mean age was 63±12 years;29 patients were male;1 case had Marfan syndrome. The median time from onset to extracorporeal circulation initiation was 5 hours (range 2~51). Postoperative extracorporeal membrane oxygenation (ECMO) was used in 5 cases;in-hospital mortality occurred in 8 cases;and 8 cases had residual sequelae of cerebral infarction (controlled reperfusion in 1).
Conclusion:Strategies for treating coronary malperfusion require improvement. In cerebral malperfusion, controlled reperfusion may be effective, with fewer residual sequelae in treated cases.
© Nankodo Co., Ltd., 2026

