Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
- 参考文献 Reference
- サイト内被引用 Cited by
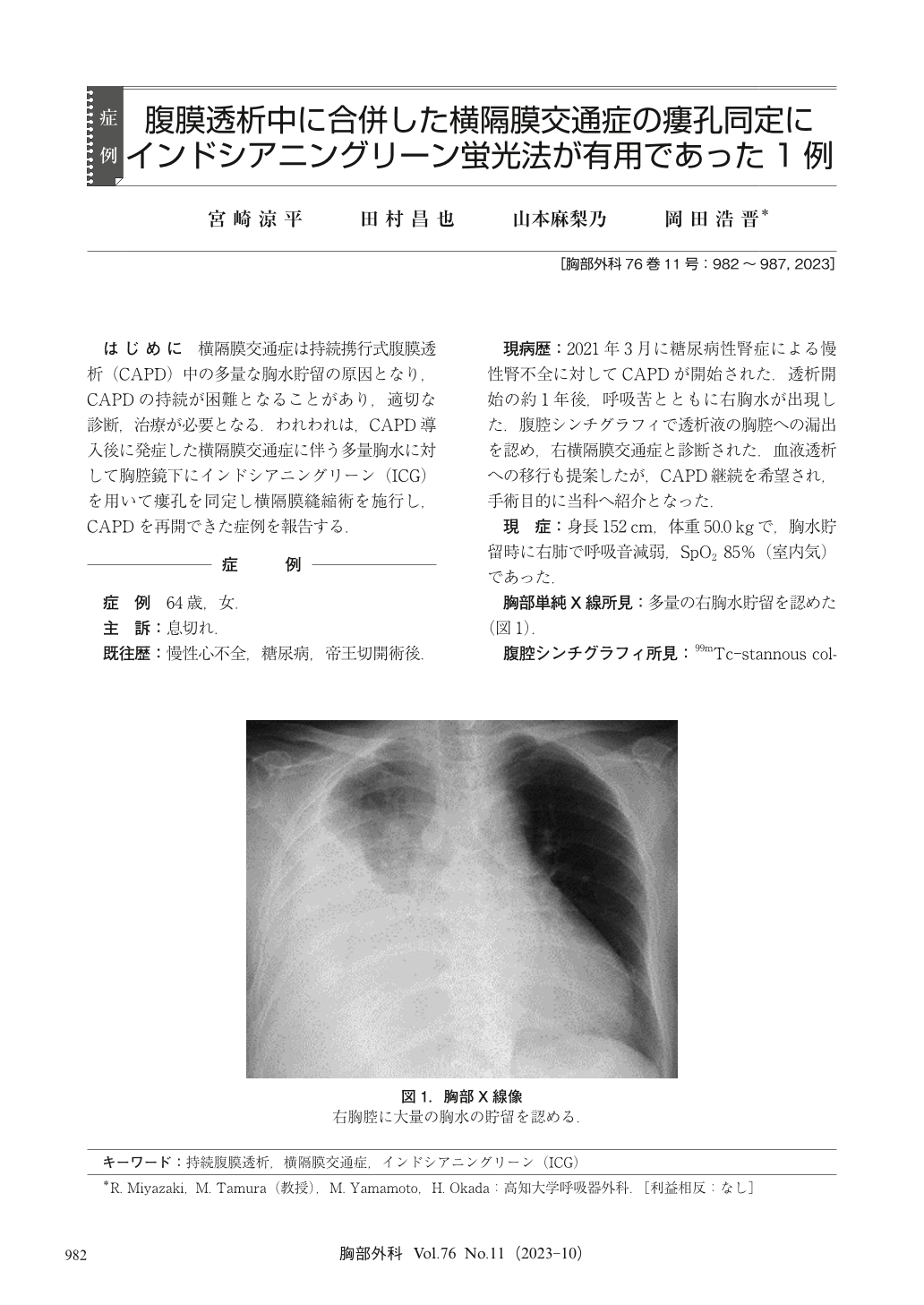
はじめに 横隔膜交通症は持続携行式腹膜透析(CAPD)中の多量な胸水貯留の原因となり,CAPDの持続が困難となることがあり,適切な診断,治療が必要となる.われわれは,CAPD導入後に発症した横隔膜交通症に伴う多量胸水に対して胸腔鏡下にインドシアニングリーン(ICG)を用いて瘻孔を同定し横隔膜縫縮術を施行し,CAPDを再開できた症例を報告する.
A 64-year-old female with chronic renal failure had been receiving continuous ambulatory peritoneal dialysis (CAPD). She developed acute hydrothorax in the right pleural cavity 1 year after the commencement of CAPD. Scintigraphy revealed a diagnosis of pleuroperitoneal communication, and we performed video-assisted thoracoscopic surgery. We infused a dialysis solution containing indocyanine green (ICG) through CAPD catheter. Near-infrared fluorescence thoracoscopy revealed a fistula that could not be identified by white light. We sutured the fistula covered with a polyglycolic acid sheet and fibrin glue. The CAPD was able to be resumed 8 days after surgery, and there was no recurrence of pleural effusion 10 months since surgery. Identification of the diaphragmatic fistula is important in the treatment of pleuroperitoneal communication. This technique using near-infrared fluorescence thoracoscopy with ICG was useful in identifying the fistula, and it emitted sufficient fluorescence even at low concentration ICG.
© Nankodo Co., Ltd., 2023

