Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
- 参考文献 Reference
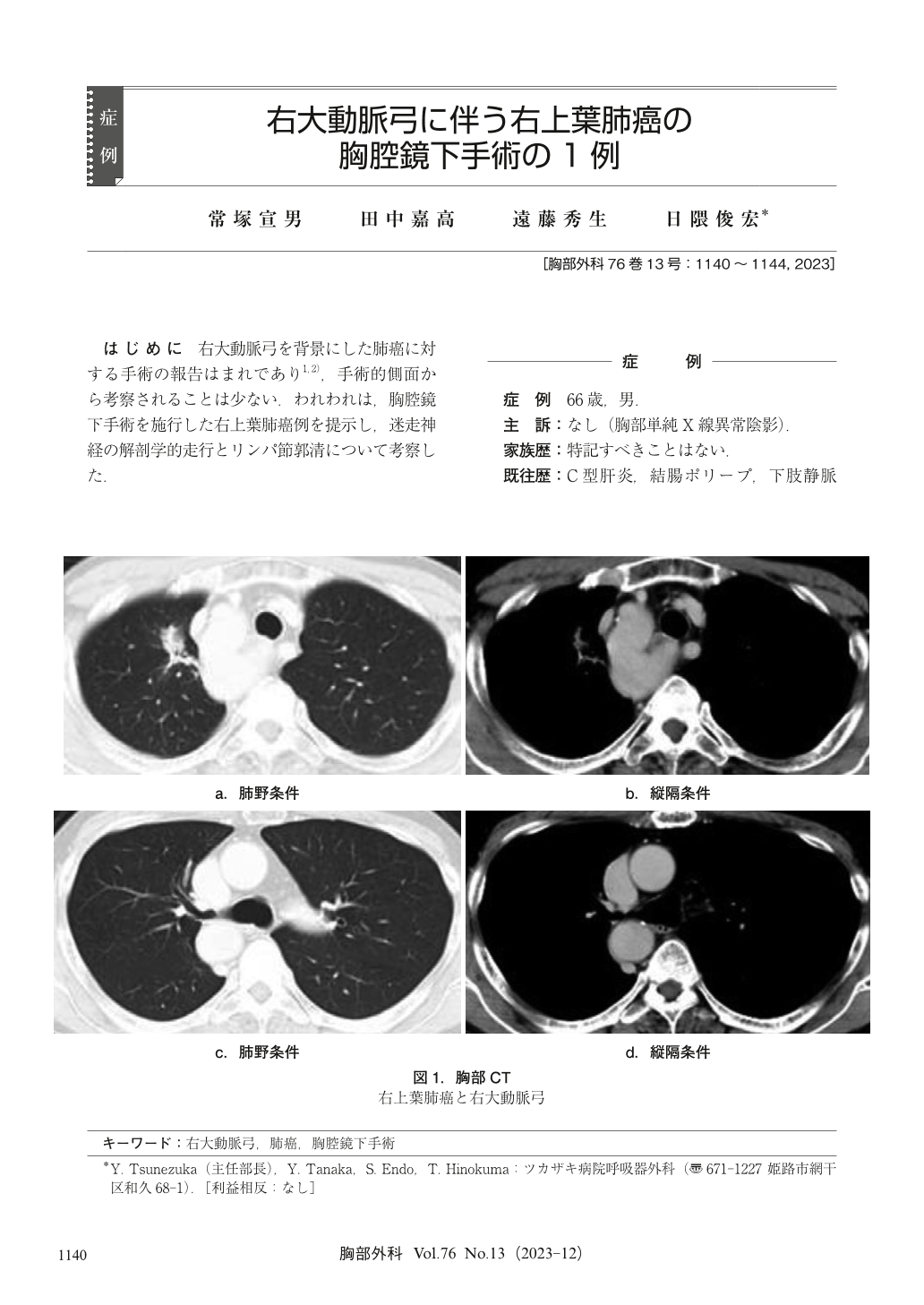
はじめに 右大動脈弓を背景にした肺癌に対する手術の報告はまれであり1,2),手術的側面から考察されることは少ない.われわれは,胸腔鏡下手術を施行した右上葉肺癌例を提示し,迷走神経の解剖学的走行とリンパ節郭清について考察した.
It has been reported that the recurrent nerve may not be recognized during mediastinal lymph node dissection in surgery for right upper lobe lung cancer associated with the right aortic arch. In the present case, a 66-year-old man underwent thoracoscopic right upper lobectomy for right upper lobe lung cancer associated with the right aortic arch. The gap between the superior vena cava and descending aortic arch was narrow, and the vagus nerve ran between the superior vena cava and the aorta. The recurrent laryngeal nerve was able to confirm. The vagus nerve ran the hilum of lung back side from arch of azygos vein on the peripheral side. The morphology of the right aortic arch varies from case to case, and if the vagus nerve and recurrent nerve are difficult to identify, the nerve may be hidden by the superior vena cava. If the nerve cannot be recognized, the space between the superior vena cava and the aorta should be dissected and confirmed. In addition, taping the vagus nerve and observing it from the caudal to the cephalic side may be useful for the recurrent nerve that turns to the mediastinum. In this case, magnification of the thoracoscope is extremely useful.
© Nankodo Co., Ltd., 2023

