Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
はじめに
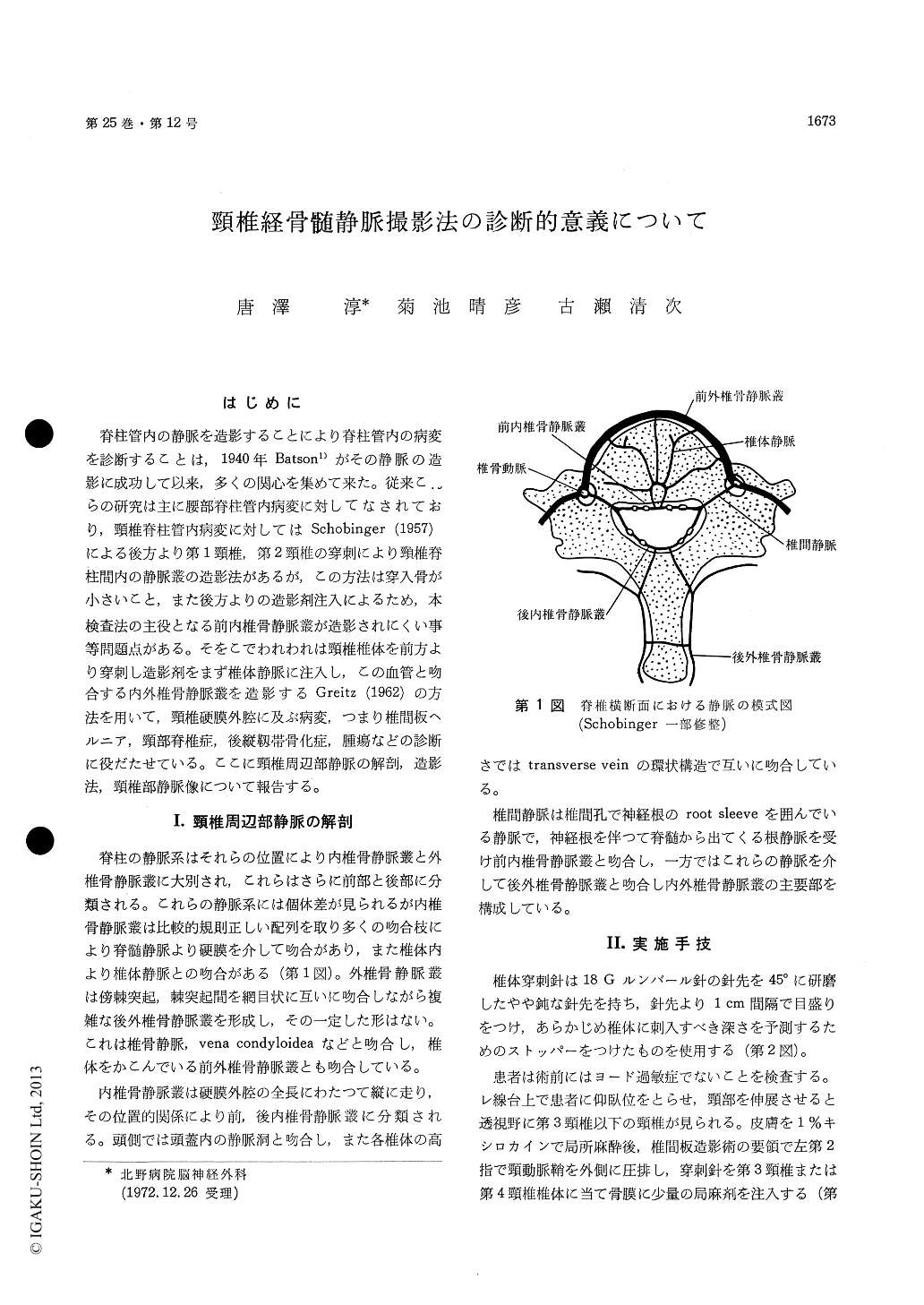
脊柱管内の静脈を造影することにより脊柱管内の病変を診断することは,1940年Batson1)がその静脈の造影に成功して以来,多くの関心を集めて来た。従来これらの研究は主に腰部脊柱管内病変に対してなされており,頸椎脊柱管内病変に対してはSchobinger(1957)による後方より第1頸椎,第2頸椎の穿刺により頸椎脊柱間内の静脈叢の造影法があるが,この方法は穿入骨が小さいこと,また後方よりの造影剤注入によるため,本検査法の主役となる前内椎骨静脈叢が造影されにくい事等問題点がある。そをこでわれわれは頸椎椎体を前方より穿刺し造影剤をまず椎体静脈に注入し,この血管と吻合する内外椎骨静脈叢を造影するGreitz(1962)の方法を用いて,頸椎硬膜外腔に及ぶ病変,つまり椎間板ヘルニア,頸部脊椎症,後縦靱帯骨化症,腫瘍などの診断に役だたせている。ここに頸椎周辺部静脈の解剖,造影法,頸椎部静脈像について報告する。
In making a diagnosis of intraspinal canal lesion, we use a method to visualize the cervical venous plexus by puncturing the cervical vertebral body from the front followed by the injection of a contrast medium (Greitz's method). A puncture needle used is a 18G Lumbal needle with the scale of 1 cm interval with the pointed head grinded at 45° which is equipped with a stopper to preestimate the depth of puncture into the vertebral body. The serial angiopraphy was performed by use of 8 ml of 60% Conray. By puncturing the C3 or C4 vertebral body, all cervical venous slexus could be visualized. After the upper margin of the lesion was visualized by the puncture of the uppercervical vertebral body, the lower margin of the lesion was observed by the retrograde filming following the puncture of the lower cervical vertebral body, and thus the range of the legion could be recognized.
We have so far carried out this method 26 times in 22 patients with spinal tumor, cervical spondylosis, calcification of the posterior longitudinal ligament, Klippel-Feil syndrome and traumatic cervical syndrome. Complex venous plexus at the site of the spinal canal often makes the interpretation of the roentgenogram difficult, so that the cervical intraosseous phlebography from another direction is necessitated. In this sense, if the cervical vertebra is effaced by means of the substruction technique, the diagnostic value is enhanced. Laminagraphy, to a certain extent, dissolves a problem of ambiguity in the filming presented by the head shadow in the anteroposterior view, by the shoulder shadow in the lateral view and by the overlap of the vein, and at the same time clarifies abnormal shadow of the internal vertebral venous plexus and the intervertebral vein. As changes in the venous picture necessary for the diagnosis of the cervical legion, there are two signs ; one is a direct sign presented by the internal vertebral venous plexus and the intervertebral vein, and the other is an indirect sign presented by the external vertebral venous plexus. The anterior internal vertebral venous plexus existing in the epidural space is directly oppressed by the legion extending to the extradural space, and thereby displacement of the venous plexus, narrowing, occlusion and enlargement are caused (direct signs). The circulation disturbances in the anterior internal vertebral venous plexus transmit the contrast medium injected into the vertebral vein, the external vertebral vein and the jugular vein, and thus indirect signs are presented. As far as those who underwent operation in our subjects were concerned, reexamination of the legion was conducted in all of them by means of mielography, and consequently, it was found that there were no cases which showed findings different from those of intraosseous phlebography. In executing the present method, there appear occasionally some cases which present abrupt venous enlarement at the time of the injection of a contrast medium and complain of shoulder pain for a little while, but the severity of the pain is not so serious.
We wish to emphasize that the present method is easy and safe to perform, and is advantageous for its high diagnostic value. And we hold that this method is excellent as a screening test to be conducted in out-patients, and as a test that can be repetitively carried out for diagnostic observation.
Copyright © 1973, Igaku-Shoin Ltd. All rights reserved.

