Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
本学麻酔科では従来より胸郭外陰圧式人工呼吸,negative extra-thoracic pressure ventilation (以下,NETPV)の研究・開発に取り組んでいる1,2)。NETPVは気管内挿管の必要がないため,気管内チューブの留置にともなう会話や経口摂取の制限,患者の行動制限などがもたらす精神的・肉体的苦痛を伴わずに人工呼吸が可能である。
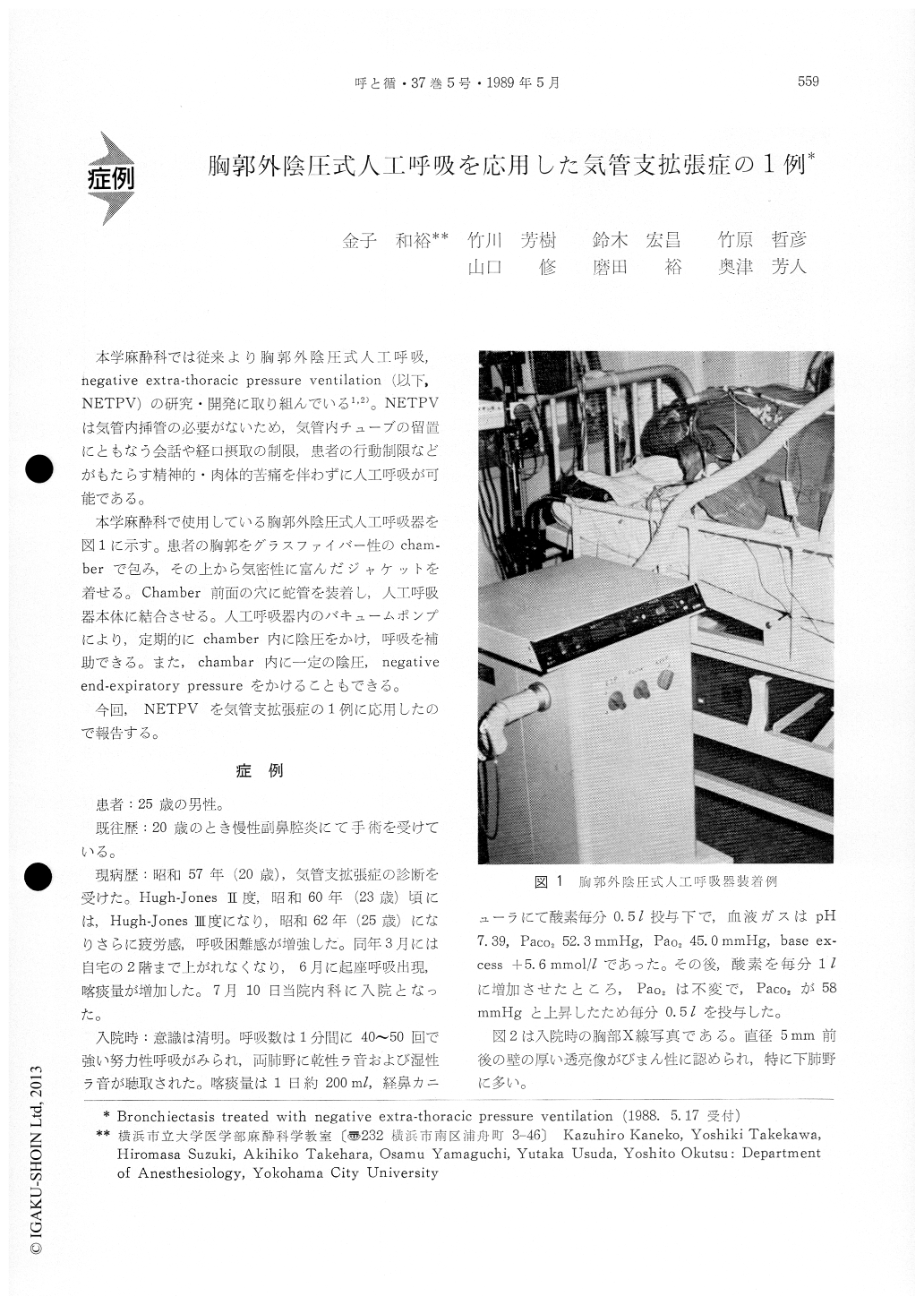
本学麻酔科で使用している胸郭外陰圧式人工呼吸器を図1に示す。患者の胸郭をグラスファイバー性のcham-berで包み,その上から気密性に富んだジャケットを着せる。Chamber前面の穴に蛇管を装着し,人工呼吸器本体に結合させる。人工呼吸器内のバキュームポンプにより,定期的にchamber内に陰圧をかけ,呼吸を補助できる。また,chambar内に一定の陰圧,negativeend-expiratory pressureをかけることもできる。
A 25-year old man with 5-year history of bron-chiectasis was admitted to the ICU complaining of severe shortness of breath. He had a respiratory rate of 40 to 50 breath/min. On 0.5 l/min of oxy-gen with nasal cannula, arterial blood pH was 7. 39, PaCO2, 52.3 mmHg, PaO2 45.0 mmHg. Then, on 1 // min of oxygen, PaO2 was unchanged, but PaCO2 increased to 58 mmHg. As his consciousness was so clear, we applied to him the negative extra-thoracic pressue ventilator which was designed by the aut-hors. Negative extra-thoracic pressure ventilation (NETPV) was maintained at a IMV rate of 30 bre-ath/min, peak negative extra-thoracic pressure of -20 to -30 cmH2O, and an inspiratory/expiratory ratio of 1:2. During NETPV, his respiratory rate and oxygen consumption were decreased and PaO2 was increased compared with his spontaneous brea-thing. He made a recovery from dyspnea, especially, he was able to take a deep breath. When NETPV was applied to him, pulmonary artery and arterial catheterizations revealed that central venous pressure was slightly decreased, cardiac index unchanged or slightly decreased, heart rate, systemic blood pres-sure, and pulmonary arterial pressure unchanged compared with spontaneous breathing. The patient was able to read books and maintained communica-tion in his voice with his family and the medical staff. After 3 days of the treatment with NETPV, a marked improvement,was noted and the patient was discharged from the ICU.
NETPV has the benefits as follows. First, it isvery easy for both a patient and a doctor to assist his breathing because an endotracheal intubation is not necessary. Second, we can increase Flo, without a fear of CO2 narosis as the patient's breathing is as-sisted. Third, patient's oxygen consumption is dec-reased, and subsequently respiratory muscle fatigue can be prevented. So, NETPV can be very useful in the treatment of mild respiratory distress.
Copyright © 1989, Igaku-Shoin Ltd. All rights reserved.

