Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
はじめに
Kenamore1)(1940年),Benedict2)(1948年)などにより初められた直視下胃生検は,Hirschowitzら3)(1958年)によるFiberscopeの開発につづき,これを用いた直視下生検法が初められ4)~7),その後本器の改良と手技の進歩により胃癌の生検がようやく臨床的に可能となった7)~13).
現在X線,内視鏡,細胞診とならんで術前の唯一の組織診としての生検が早期胃癌診断のために欠くことのできないルチーン検査法の1つとなった14)15).
ある程度の拡がりをもった早期胃癌病巣からの生検採取は比較的容易であったが,微小な病巣からの生検採取は必らずしも容易でなかった.しかし,最近生検用ファイバースコープの改良と技術の進歩により比較的小さな早期胃癌病巣からの生検も可能となってきた.
本稿においては最大径1cm以下の微小早期胃癌の直視下胃生検について,その成績と手技を述べる.
Out of 140 cases (145 lesions) of proven early gastric cancer, 136 cases (139 lesions) or 97.1% (95.9%) were diagnosed as cancer by gastric biopsy.
The size of 28 lesions of small early gastric cancer or 19.3% in 145 early gastric cancer lesions, consisting of 16 of Ⅱc, 8 of Ⅱa+Ⅱc, 2 of Ⅱa, one of Ⅱc + Ⅱb I and respectively, was macroscopically less than 2cm in largest diameter, and the size of 12 lesions of minute early gastric cancer among those cases, consisting of '7 of 3 of IIa+IIc and 2 of Ⅱa, was macroscopically less than 1 cm in largest diameter.
Eight lesions in 7cases of minute early gastric cancer, in which histological extent of cancer was less than one cm in diameter, were biopsied. They consisted of 5 lesions of Ⅱc, 2 of Ⅱa and one of IIa+IIc. Among those, 6 lesions or 75% were correctly diagnosed as cancer by biopsy.
It was found as general tendency that accuracy of gartric biopsy went gradually down in inverse proportion to the size of the lesion.
However, negative results of biopsy were not solely due to the size of the lesion, but also in a far greater measure to its location, inefficient instruments and unskilled examiner.
In two cases of negative biopsy of minute early gastric cancer, the lesions were both located on the lesser curvature of the antrum. In one case biopsy was performed with fibergastroscope for biopsy without angle mechanism in our early series of the study. Although the lesion was observed endoscopically, one failed to obtain cancer tissue because the biopsy forceps were unable to reach the lesion correctly.
In the other negative case, double lesions of minute early gastric cancer were present; a Ⅱa lesion on the posterior wall of the angulus and a Ⅱa lesion on the lesser curvature of the antrum. Observation and biopsy of the Ⅱc lesion were not sufficiently performed and only one biopsy specimen was obtained from noncancerous area of the Ⅱc-like lesion because the extent of cancer histologically proved was less than that of the lesion macroscopically confirmed, although observation and biopsy of the Ⅱa lesion were sufficiently performed.
Differential diagnosis between minute early gastric cancer and ATP lesion has clinically been attained only by biopsy, because differentiating minute early gastric cancer from ATP lesion was generally difficult roentgenologically and endoscopically.
In order to obtain by biopsy correct diagnosis of minute early gastric cancer, not only should one use a fibergastroscope for biopsy equipped with angle mechanism, but also one shouid obtain biopsy specimens only after adequate observation of the lesion close front view in the center of visual field of the scope.
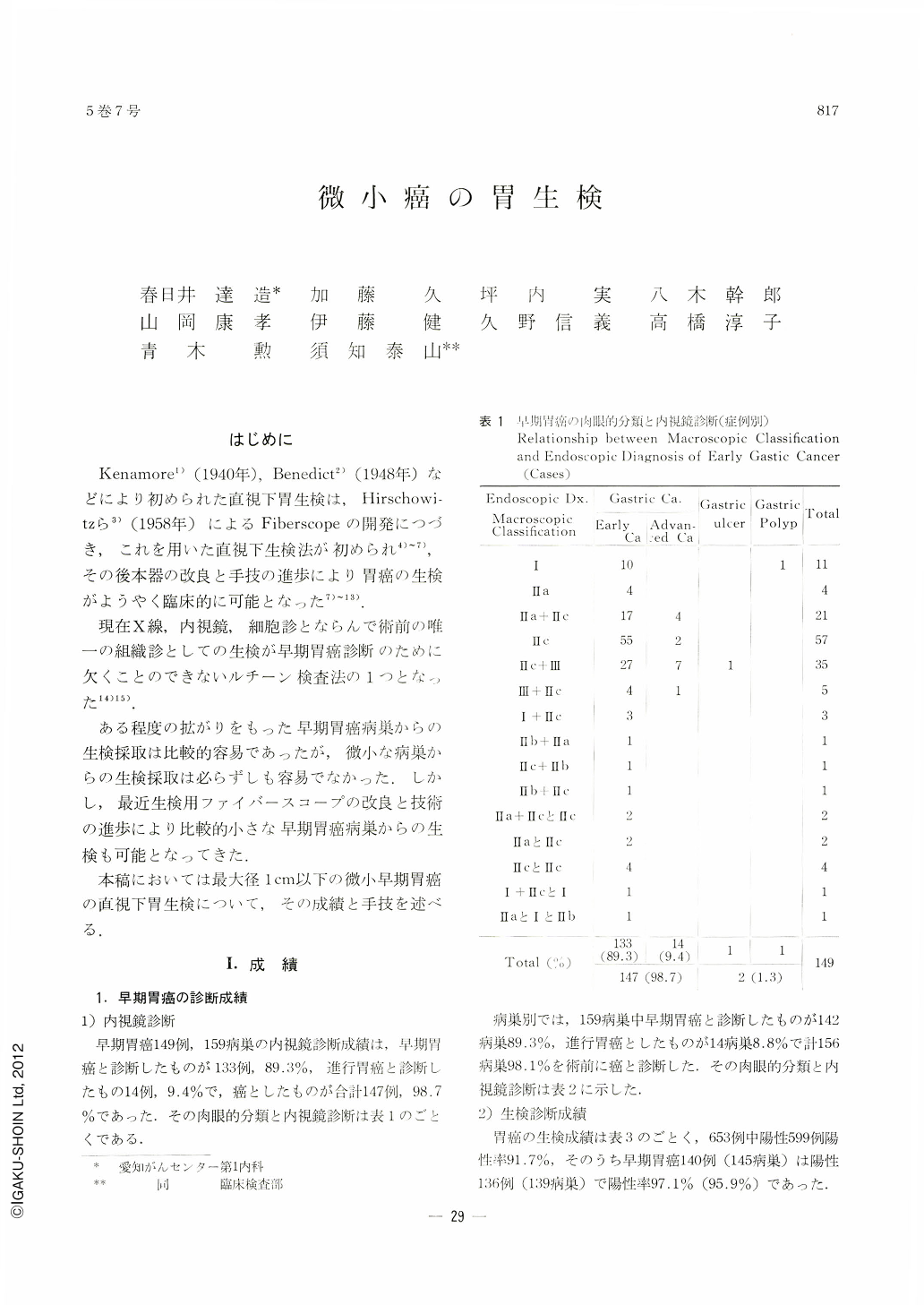
Copyright © 1970, Igaku-Shoin Ltd. All rights reserved.

