Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
胃リンパ細網細胞増殖症についてはKonjetzny(1928)8)が慢性胃炎特殊型として記載以来,その本態と組織診断基準に関し多くの報告があり1)~13),現在なお病理組織学的にも不明の一疾患単位として統一的には理解されていない.また,悪性リンパ腫との鑑別については病理組織水準においても両者の鑑別の困難な症例があり,そのような報告が少なくない.
われわれは臨床諸検査の段階で悪性リンパ腫と診断し,組織学的にLymphoreticular hyperplasiaを主体とした病変中に散在性あるいは小集簇性に細網細胞の異常増生を認め早期細網肉腫への移行を強く疑わせる症例を経験した.
A 58 year old woman has suffered from epigastric pains after cholecystectomy since 8 years ago. She was admitted with a 4 months continued epigastric pain, and weightloss of 10 kg within recent 2 months. Double contrast roentgenogram in admission has revealed remarkably advanced lesion in comparison with that of 4 months before admission as like as Fig. 1 and 2, 3 show. These roentgenographic and endoscopic findings were interpreted as showing malignant lesion. Cytologic diagnosis of imprint smear of endoscopic biopsies was reticulum cell sarcoma.
Under preoperative diagnosis of superficial infiltrating reticulum cell sarcoma, total gastrectomy with splenectomy was performed. Postoperative course was uneventful except of the complication of hepatitis.
In the resected stomach diffuse extended ulcerated lesion with large rugae and uneven border were seen. Gross findings could not exclude malignancy.
Histopathologically greatest part of the depressed lesion showed atrophic erosive gastritis and was covered with thin re-epithelization and small shallow (Ul-II) ulcers and slightly thicekned fibrous submucosa were seen. Gastric glands and surface epithelia have disappeared and mucosa were displaced with sheet of massive lymphoreticular tissue, composed of reticulum cells, lymphocytes and plasma cells. Massive infiltration of plasma cells were seen predominantly in upper half of the mucosa. Lymphfollicles were found sporadic, presence of reaction center was rare. This dense infiltration was located in the mucosa and not extended in submucosa.
This lesion may be ranked with Nakamura's diffuse flat form and Rousselot's polymorphic type of lymphoreticular hyperplasia.
Characteristic histological findings of this case were the presence of foci of unusual reticulum cell hyperplasia. scattered in and around the follicles. These cells had large nucleus, in some nucleus slight indentation found, one or two clear nucleoli were often seen. Cytoplasma was clear, broad and polygonal shaped. A few binucleated reticulum cells were present in slight degree. In some part of reticulum cell proliferation eosinophilic cells were seen, but Hodgkin's cell was not found.
In some area, remained small number of surface epithelia were surrounded with conspicuously proliferated large clear cells. These large clear cells were not stained through PAS, alcian blue and mucicarmin, ultrastructually were immatured cells and did not show the features of epithelial origin. Microscopically and ultrastructually transition from epithelial cells to this large clear cells could not be observed. Foci of conspicuously proliferated reticulum cells were plotted in Fig. 13. Most of them were situated in the edge of depressed lesions but also scattered diffusely in the body of the stomach.
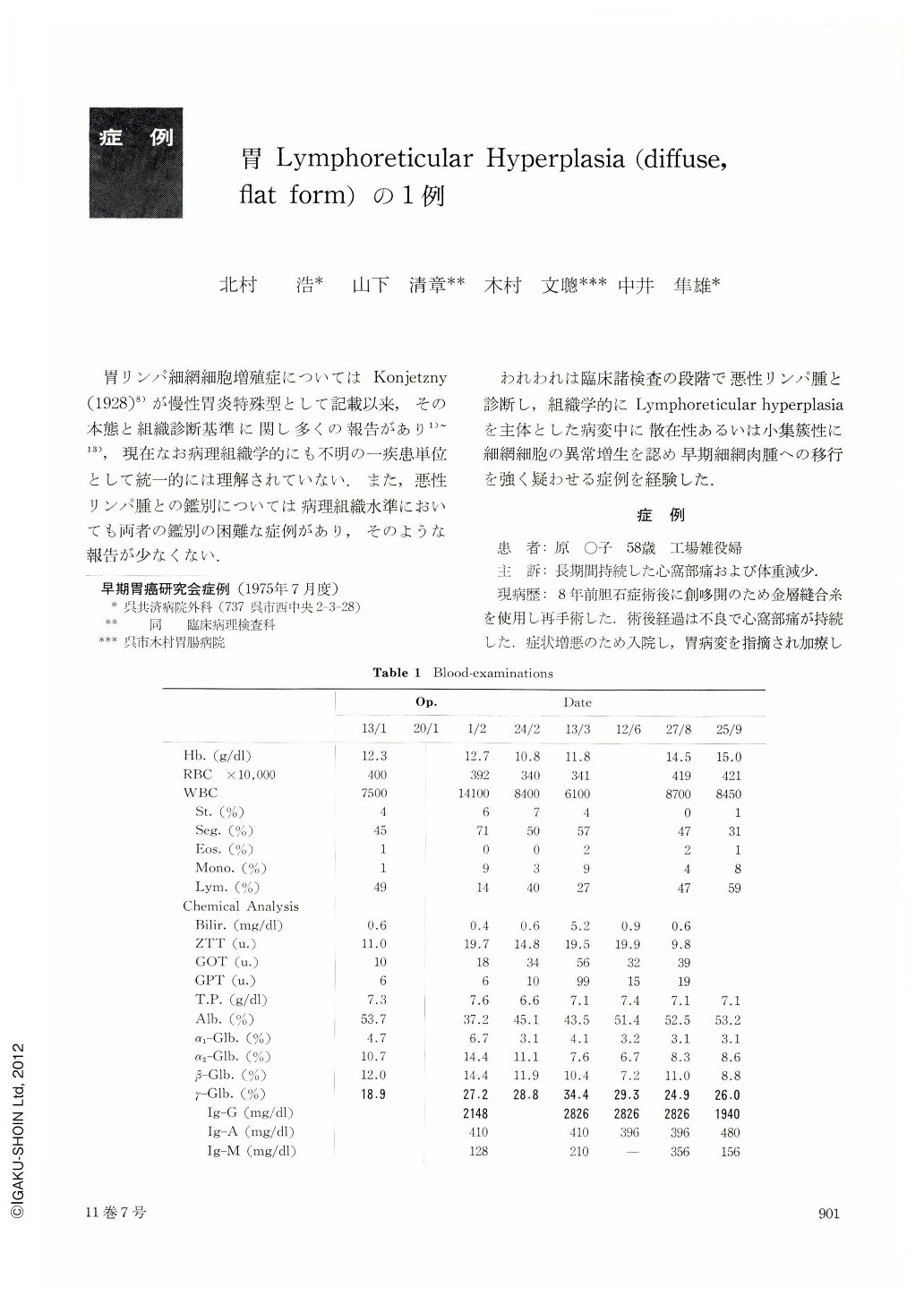
This gastric lesion may be caused by recurrent erosive gastritis and excessive reaction of gastric lymphoreticular tissue, but inducing factor of such excessive lymphoreticular hyperplasia was in mystery. But in this case Gamma-globulinemia and high Ig-G value had been observed, then it was supposed some kind of repeated antigen stimulation caused this lesion.
The presence of many inflammatory cells in proliferated foci and absence of massive monotonous proliferation of reticulum cells were rather negative factors for the conclusion of reticulum cell sarcoma. But precise differentiation with reticulum cell sarcoma was impossible even with the histopathological findings.
Follow-up of this patient is essentially necessary.
Copyright © 1976, Igaku-Shoin Ltd. All rights reserved.

