Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
はじめに
胃隆起性病変が,内視鏡的に良性であるか悪性であるかを判断する揚合,ある程度以上の大きさをもつBorrmann Ⅰ型の胃癌や,かなり特徴的な形態を呈するⅡa+Ⅱc型の早期胃癌についてはさほど診断が困難ではない.しかしながら,比較的病巣の小さいⅠ型早期癌は,Ⅱa型とともに良性の隆起性病変との判別が困難な場合にしばしばそう遇する.
内視鏡検査技術の進歩とともに,直視下胃生検も今日では広く行なわれるようになり,内視鏡検査時に疑わしい所見が見られた場合,引続いて直ちに胃生検を行なうのが一般的なすう勢になろうとしている.しかしながら,より確実な内視鏡的悪性指標の追求が病変の経過観察に大変寄与することは当然であり,胃生検はむしろ診断の確定に用いるようになるべきであろう.
今回のⅠ型早期胃癌の内視鏡的診断に関しては病変の色調,表面性状などの内視鏡所見について統計的に観察するとともに,切除肉眼標本を用いて,形状ならびに表面性状について分類し,Ⅰ型早期癌の形態的特異性の有無を検討した.
また,これらⅠ型早期癌の組織切片上からみた癌巣の局在の分析からポリープの癌化の問題についてもふれてみた.
観察に用いた症例は,本内科および関連病院での手術症例であり,その内訳はⅠ型早期胃癌9例Ⅱa型4例,および隆起を主とするⅡa+Ⅱc型早期癌10例,胃ポリープ単発12例,多発7例(32個)粘膜下腫瘍12例(隆起性肉腫2例を含む)進行癌3例,計58例82病変である.
In the endoscopic diagnosis of type Ⅰ early gastric cancer, along with type Ⅱa, it is sometimes difficult to discriminate it from benign protruding lesion. Although the role of gastric biopsy is important in accurate diagnosis of early gastric cancer, it is as important in the follow-up of a lesion to look for an index of malignancy by endoscopy.
The subjects of this study in the endoscopic diagnosis of type Ⅰ early gastric cancer were 82 lesions in 58 cases of protruding lesions of the stomach, including 9 cases of type Ⅰ early cancer. They were statistically investigated from the standpoint of endoscopic findings. Gross specimens of the resected stomachs were employed as well in their morphological classification in order to find, if any, characteristics in the shape of type Ⅰ early cancer. Lesion in situ of this variety has also been studied with some reference to canceration of gastric polyp.
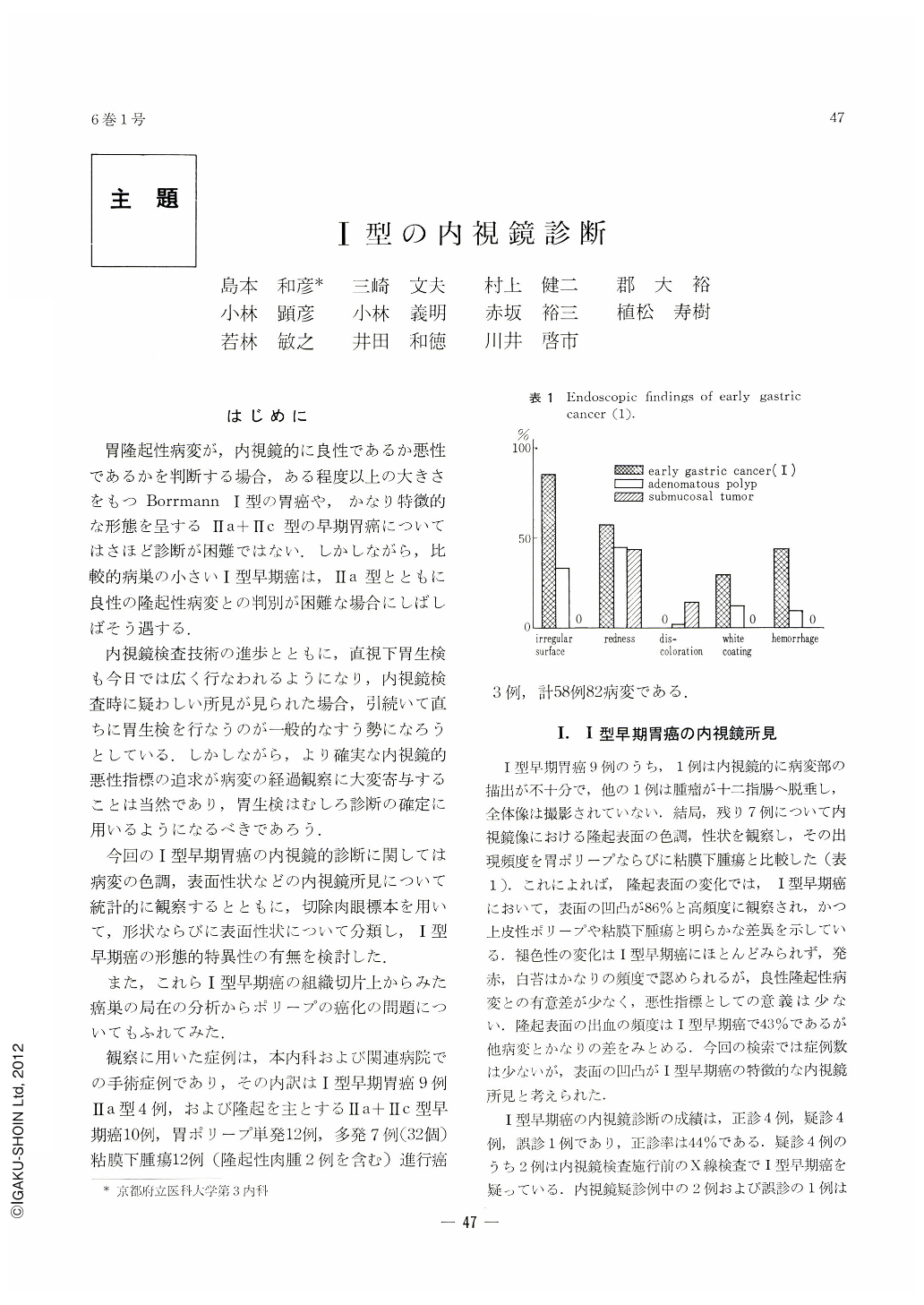
Endoscopic observation of type Ⅰ early cancer shows that, as compared with gastric polyp and submucosal tumor, it has no significant difference in the findings of engorgement and white exudate over the surface of protrusion. Ultimately, the most characteristic feature of type Ⅰ has been found to lie in the unevenness of its surface.
Protruding lesions of the stomach have been accordingly classified into three basic types: smooth elevated type, spherical type and dish-like type. At the same time, unevenness of surface has been divided into four degrees: smooth, granular, small nodular and large nodular. Analysis of these two factors has revealed that lesions of type Ⅰ early cancer all belong to spheric type; those of pedunculated type Ⅰ early cancer have marked unevenness of surface, either small nodular or large nodular. In nonpedunculated type three out of four cases show the same degree of surface unevenness. Considered from the degree of depth invasion of cancer, cases of submucosal infiltration also show more marked uneven surface as compared with those of mucosal invasion, in strong contrast with less uneven surface, either smooth or granular, seen in the majority (89 %) of gastric polyp or submucosal tumor. The size of protruding lesions is also suggestive. In type Ⅰ early cancer, four out of five pedunculated spherical type measure more than 30 mm in diameter, and three out of four sessile spherical type have the diameter of more than 20 mm. On the other hand, 38 out of 42 cases of benign protruding lesions of spherical type are only less than 20 mm in diameter. For this reason, the size of protruding lesion is as important as the above-mentioned two factors, i.e., its form and unevenness of surface, in discriminating malignant lesion from benign one.
The extent of cancer spread in the cut surface of protruding gastric cancer including type Ⅰ early one has also been studied with the result that fountainlike protrusion of the muscularis mucosae, remaining pyloric glands, and localized existence of cancer within the tumor, three outstanding characteristics considered by the authors as essential for cancerated polyp, have not been fully met with, so that the rate of canceration of gastric polyp is considered as very low.
Copyright © 1971, Igaku-Shoin Ltd. All rights reserved.

