Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
膵癌の症例に血管造影を行なうと,そのほとんどはhypovascularで,腫瘍濃染像や造影剤のpoolingを示すことは稀で,血管造影所見としては動脈のencasement,閉塞としてみられることが多い.したがって腹腔動脈と上腸間膜動脈を造影するだけでは小さな膵癌の診断は困難な場合が多く,superselective angiographyが必要である.また門脈系をarterial portographyによって描出するか否かも血管造影の膵癌診断能に関係がある.
膵癌の血管造影の診断能についてはすでに多数の報告がある1)~18).これらの報告のうち膵癌の大きさと血管造影の診断的中率について記載されているものは少数にすぎない.その上,血管造影の手技が一定しないのでどのような方法でどの程度までこまかい動脈を造影した結果の診断能であるかもはっきりしない.本邦では多数の施設で血管造影が行なわれているが,その施行方法が一定していないのが現状である.
Ⅰ. Material
Thirty two cases pancreatic carcinoma histologically confirmed by operation or autopsy were classified into two groups in regard to their location. In 19 cases, the tumor involved the head and in 13 cases the lesion involved body and/or tail of the pancreas. The ratio of male to female is 23: 9. Age ranges from 45 to 80 years with an average of 60 years. Of the 32 cases of pancreatic carcinoma, 31 of cases (96%) were accurately diagnosed by angiography preoperatively. Eight of cases located in the head, 1 case in the body and 1 case in the tail were resectable, accounting for 10 cases or 31% in all. Of the 10 cases which had undergone resection, 6 cases were regarded as small carcinoma less than 2 cm in diameter.
Ⅱ. Method
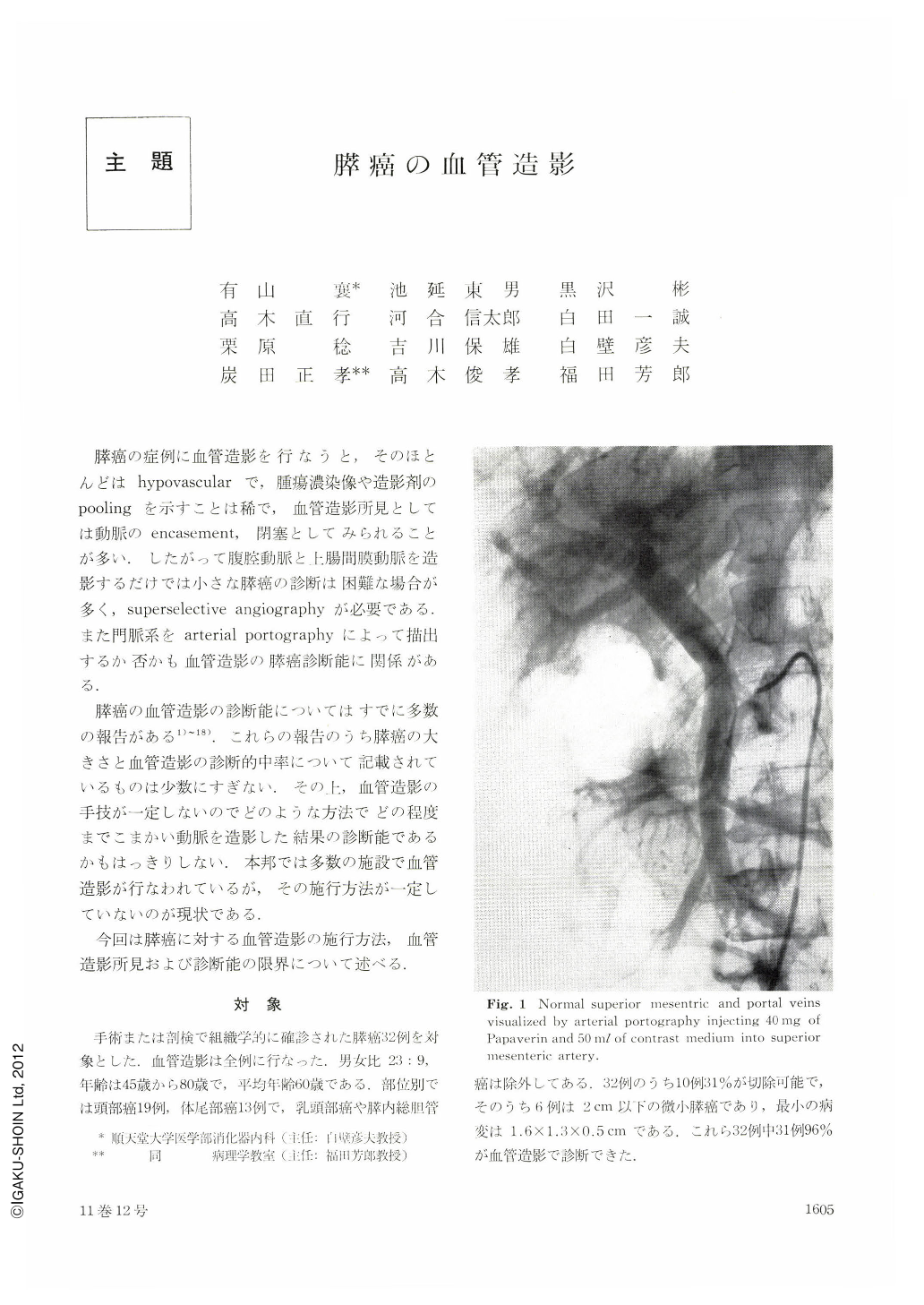
In performing angiography, a large quantity of contrast medium (50 ml of iodamide meglumin 65%) and vasodilator (Papaverin 40 mg) are, first of all, used for arterial portography in order to visualize the portal system. This procedure meets the required purpose of being one of the decisive vehicles regarding resectability by confirming the extent of infiltration of carcinoma (Fig. 1, 15, 16, 17).
There are many instances of imcomplete and inaccurate diagnosis of small pancreatic carcinoma when only celiac and superior mesenteric angiography are performed. The pancreatic carcinoma with encasement of the larger arteries surrounding the pancreas is inoperable. Thus, superselective angiography is indispensable for diagnosing small pancreatic carcinoma. Superselective angiography will be successful in most cases by using a catheter exchanging method or Cope-Eisenberg system. For the carcinoma in the head of the pancreas, superselective angiography of the gastroduodenal artery or of the pancreatic arcade should be performed. For the carcinoma in the body or tail of the pancreas, superselective catheterization of the dorsal pancreatic or splenic arteries should be done. Complete visualization of pancreatic arteries will be achived by combining a high bolus injection of contrast medium directly into pancreatic artery (Fig. 2, 3).
Ⅲ. Angiographic Findings of Pancreatic Carcinoma
Angiographic findings of pancreatic carcinoma is accounted for in Table 1. Most of carcinomas are poorly vascularized and no tumor stain is observed. From the study of injecting barium sulfate into artery of resected specimen, hypovascularity of pancreatic carcinoma is obvious (Fig. 4~10). Thus, important findings of pancreatic carcinoma are arterial encasement and occlusion. Venous changes are nonspecific. If intrapancreatic small vessel bed is well demonstrated by angiography, very small pancreatic carcinoma can be diagnosed (Fig. 11~14). The smallest lesion diagnosed in present series was 1.6×1.3×0.5 cm and was located in the body of the pancreas. In small pancreatic carcinoma, arterial and venous changes are confined to intrapancreatic vessels. Angiograpic findings of 6 cases of small pancreatic carcinoma less than 2 cm in diameter is shown in Table 2.
Ⅳ. Prediction of Resectability of Pancreatic Carcinoma
A clear demonstration of not only arteries but also of the portal system is necessary in predicting resectability of pancreatic carcinoma. The required standards for the prediction of resectability are as follows:
1. Encasement should be confined to intrapancreatic arteries.
2. No invasion of portal or superior meseteric veins.
3. No presence of metastasis.
Ⅴ. Evaluation of Angiography in the Diagnosis of Pancreatic Carcinoma
The relative efficacy of percutaneous transhepatic cholangiography (PTC), endoscopic retrograde cholangiopancreatography (ERCP) and angiography was studied in 32 individuals with proven pancreatic carcinoma (Table 4). PTC is suited to demonstration of malignacy in the head of the pancreas, however, it has no diagnostic potentiality in cases of carcinoma without jaundice especially tumor in the body or tail of the pancreas. Advantage of PTC is the drainage which facilitates safely the patient's jaundice reduction and improvement of general status. ERCP is the most reliable method for detecting pancreatic carcinoma, however, the size, extent and resectability of carcinoma can not be decided (Table 5). Thus, most effective combination of examinations in the diagnosis of pancreatic carcinoma is ERCP and angiography. Detection of pancreatic carcinoma can be carried out by ERCP, and angiography accurately defines the size, extent and resectability of the tumor. Also differentiation of chronic pancreatitis from pancreatic carcinoma can be diagnosed by angiography (Table 3). The angiogram is useful at the time of operation. Faulty assessment of tumor site and size might lead to incomplete resection. In order to prevent such incidents, a detailed angiographic evaluation of tumor size and vascular anatomy is a most, making it possible to map out the area to be resected exactly.
Ⅵ. Conclusion
Thirty one out of 32 pancreatic carcinoma (96%) were correctly diagnosed preoperatively by angiography. Capability of angiography to diagnose lesion is as small as 1.5 cm. In order to diagnose small malignancy of the pancreas, entire intrapancreatic vessel bed must be visualized. Combination of angiography and ERCP is the most effective for the diagnosis of pancreatic carcinoma.
Copyright © 1976, Igaku-Shoin Ltd. All rights reserved.

